Identical twins shared huge impact after one used botox for 20 years and other didn’t
Botox can have long lasting impacts
A set of identical twins shared the huge impact after just one of them used Botox for 20 years.
The pair of sisters were part of a scientific study that saw one of them undergoing a series of injections across the two decades. Known medically as botulinum toxin, Botox is a prescription drug that can also be used for cosmetic procedures.
It might get a bit of bad rep from those who don’t quite understand what it is (or aren’t sure of the differences between plastic surgery, Botox and filler) but it can make a big difference to people’s lives.
As well as reducing wrinkles and fine lines, the injections can be used to treat thing like muscle stiffness and spasms, migraines and excessive sweating. And those physical differences can be very distinct – as a doctor found when she injected only one half of her face.
This is what the twins looked like at the start of the study (American Medical Association)
The set of twins were followed for nearly two decades, with the ‘Botox twin’ undergoing injections in her forehead and between her eyebrows two to three times a year since the age of 25.
She also had some injections in her crow’s feet (those little lines that form on the outer corners of the eyes).
With Dr William Binder being behind the injections, the first resulting photos were taken in 2006, when the women were 38. And they showed that the Botox twin had more smoothness on her skin with less wrinkles compared to her sister’s more prominent crow’s feet when she smiled as well as lines on her forehead.
But a much bigger visible difference came six years later in a follow-up.
The non-Botox twin had a noticeably wider jaw, as well as a puffier visage, though it was unknown if this was related to the prescription drug.
Both women stated during that that they used sunscreen which helps to eliminate the possibility of wrinkles being caused by exposure to the sun’s UV rays over long periods of time.
The twin on the right took regular injections of Botox (American Medical Association)
It’s also noted that they both had healthy lifestyles and hadn’t been using retinols for their wrinkles but they did live in different countries.
The non-Botox woman lived in Munich while her twin lived in Los Angeles with a higher UV index.
Dr Binder wrote in the study that long-term Botox treatment can help to prevent the development of wrinkles, ‘not only by inhibiting the patient’s ability to contract the target muscle but also perhaps through behavioural modification’.
The study concluded: “Long-term treatment with Botox can prevent the development of imprinted facial lines that are visible at rest. Botox treatment can also reduce crow’s feet.
“Treatment is well tolerated, with no adverse events reported during 13 years of regular treatment in this study.”
The Dr who injected one half of her face
The un-injected side was a lot more mobile than the one which had been blasted with Botox two weeks earlier. (Instagram/@drbitafarrell)
Dr Bita Farrell decided to be a bit of a ‘lab rat’ to show just how much difference Botox can make.
With over 20 years of injecting experience, the board-certified physician injected the lower muscles on the right side of her face.
Dr Farrell explained she had targeted the DAO muscle, which pulls down the corners of the mouth, and the platysma muscle, which contributes to facial expressions and mouth movements.
“Now for you, two weeks later, I present my results as I try and contract my lower face muscles,” the California-based content creator told social media users.
She could clearly be seen struggling to get any movement out of the right side of her face, while the left side was far more expressive.
“You can see that the platysma muscle on this [left] side is really contracting and pulling my jawline down, and so is my DAO, pulling the corner of my mouth down,” Dr Farrell said.
Referring to her right side, which she injected with Botox a fortnight earlier, she added: “I’m really trying to pull this side!”
Speaking of the difference between each side, she said of the injected area: “See that this cheek rides a bit higher, this nasal labial fold seems softer and so does my shadow at the marionette on this side.”
She explained just how this has an impact: “Muscles of the face either pull up or pull down. When the muscles that pull the lower face down (platysma and DAO) are injected and relaxed with a Neuromodulator such as Botox, the muscle that pulls the mid face up (zygomaticus or cheek muscle) dominates and pulls the face up!
“This can help reduce the appearance of marionette lines, jowls, frown (rbf, or sad face), and the nasolabial folds. It also lifts the neck and can sharpen the jawline and make the cheeks appear a bit fuller and more lifted.”
Featured Image Credit: American Medical Association
Human Horns: A Brief History of Strange Growths from Heads
Dr. Pimple Popper Removes A Potentially Cancerous Horn from a Woman’s Head
While the image of humans growing horns might seem like a science fiction scenario, some individuals are experiencing the development of bony growths at the back of their skulls, often referred to as “horns”. These growths, also known as enthesopathies or insertional tendinopathies, are essentially bone spurs caused by chronic stress on the tendons and ligaments at the base of the skull.
What causes these “horns”?
Poor Posture:
The primary driver appears to be the forward head posture adopted when using digital devices (phones, tablets, etc.). This posture shifts weight from the spine to the muscles and tendons at the back of the neck, causing the bone to respond by growing.
Tendon and Ligament Stress:
The constant pulling of tendons and ligaments at the back of the head to maintain a neutral head position leads to the bone thickening and forming spurs at the attachment sites.
Why are they called “horns”?
The term “horn” is used because the bony growths can sometimes resemble horns in their shape and size. Some individuals have developed growths large enough to be visible, even under hair.
Are these “horns” dangerous?
While the growths themselves are generally benign, they are a sign of chronic stress on the musculoskeletal system. The underlying cause, poor posture and the resulting muscle strain, can lead to other issues like headaches, neck pain, and restricted movement.
How to address this issue?
Improve Posture:
Practicing good posture while using digital devices and throughout the day is crucial.
Strengthen Neck Muscles:
Exercises to strengthen the neck and upper back muscles can help support proper posture and reduce strain.
Take Breaks:
Regularly taking breaks from prolonged device use to stretch and move around can help alleviate stress on the neck and back.
What is a cutaneous horn?
A cutaneous horn is a growth on the skin that occurs due to excessive keratin growth. A cutaneous horn has numerous possible causes, ranging from skin infections to cancer.
Cutaneous horns are lesions that develop on the skin from an overgrowth of keratin. This is the protein responsible for making hair, nails, hoofs, and horns. An overgrowth of this protein is called hyperkeratosis.
The lesions usually develop in areas frequently exposed to the sun. About 60%Trusted Source of all cutaneous horns are benign, while others are cancerous or precancerous. Because of this, anyone who develops a cutaneous horn should seek medical attention.
Below, we explore the causes and risk factors for cutaneous horns, as well as how to identify one and when to contact a healthcare professional.
Causes and risk factors
Cutaneous horns develop from excessive keratin growth on the skin, particularly in very sun-damaged areas. The growths may be harmless, precancerous, or cancerous. There may be an underlying cyst, though this is extremely rare.
In terms of cancer risk, cutaneous horns on the face are more likely to be cancerous or precancerous than those elsewhere on the body. And the risk of malignancy increases with the size of the horn.
Dr. Pimple Popper Removes A Potentially Cancerous Horn from a Woman’s Head
Symptoms
A doctor can often diagnose a cutaneous horn based on its appearance alone:
The horn-like growth on the skin’s surface is typically brownish-yellow and curved.
The growths usually appear on the face, hands, forearms, or ears.
The surrounding skin may be unchanged or slightly thickened.
The growth is usually a few millimeters or centimeters long or twice as long as the base is wide.
Rarely, cutaneous horns can grow much larger.
Rarely, more than one of these growths develop in a group.
Most cutaneous horns cause no other symptoms. However, when a horn is damaged, there may be pain or an infection.
When to see a doctor
Anyone who may have a cutaneous horn should schedule an appointment with a healthcare professional to have it evaluated for skin cancer.
People who already have a cutaneous horn diagnosis should contact a doctor if any of the following symptoms develop:
pain
an increase in the size of the horn
redness, purple, or brown skin hues at the base of the horn
the horn becoming wider than it is tall
hardening or puckering of the surrounding skin
The changes above can indicate that the horn may have become cancerous.
Associated conditions and complications
Doctors associate a range of health issues with cutaneous horns.
Many of these health conditions are noncancerous, including nevi, seborrheic keratoses, viral warts, viral skin infections, and psoriasis. The latter two require medical treatment, while the others are benign.
Another growth, called a keratoacanthoma can develop from a cutaneous horn, though this is rare. This type of growth is relatively common and often benign. It is dome-shaped and can grow up to 3 centimeters in diameter. Older people, people with lighter skin, and those with sun damage have a higher risk.
A doctor may recommend surgical removal to reduce the risk of a keratoacanthoma becoming malignant, as it can resemble squamous cell carcinoma, a type of cancer.
Below, we describe the more serious conditions related to cutaneous horns that are either cancerous or precancerous.
Lisa Has a “Horn” Coming Out of Her Head | Dr. Pimple Popper
Cutaneous horn squamous cell carcinoma
Squamous cell carcinoma is the most common skin cancer that can occur with a cutaneous horn. It develops in about 94%Trusted Source of all malignant cutaneous horn cases.
There may be a greater risk of developing squamous cell carcinoma, particularly if the cutaneous horn is larger and painful, discolored, and wider at its base.
On lighter skin tones, this discoloration may appear pink or red. On darker skin tones, this discoloration may be purple-hued, gray, dark brown, or darker than the surrounding area.
A cutaneous horn can also present as an early version of this cancer, known as Bowen’s disease or squamous cell carcinoma in situ.
Cutaneous horn basal cell carcinoma
A more rare type of cancer associated with a cutaneous horn is basal cell carcinoma. Risk factors include excessive exposure to the sun or ionizing radiation, which can comeTrusted Source from X-ray or CAT scan machines.
Age, genetics, weakened immune system, and existing scarring may also increase the risk.
Cutaneous horn melanoma
Treatment
A doctor usually orders a biopsy to determine whether a cutaneous horn is malignant. This involves taking a sample of the horn, including a piece of the base.
Cutaneous horn removal
In some cases, a doctor recommends removing the entire horn. This is especially important when malignancy is a significant concern.
In the process, the doctor takes a biopsy to check for any indications of cancer. It is rareTrusted Source for a doctor to be able to rule out malignancy without a biopsy. For this reason, a doctor will almost always request a biopsy for the horn.
Never try to remove a cutaneous horn at home. A healthcare professional needs to remove it in a clinical setting.
Additional treatment options
It is important for a doctor to determine whether a cutaneous horn is benign or potentially harmful with a biopsy before any destruction of the horn.
Anyone who then wants to have a benign growth destroyed for cosmetic reasons might consider laser therapy or electrocautery, which involves a healthcare professional using heatTrusted Source to destroy the horn’s tissue.
Once a doctor removes a cutaneous horn, the outlook is usually goodTrusted Source, even when the growth was cancerous. Most people do not need further treatment after the removal.
However, if basal cell or squamous cell cancer was the horn’s underlying cause, a person needs to have regular screening to determine whether the cancer has returned.
Summary
Cutaneous horns are hard, brownish-yellow growths on the skin. They develop due to an excessive production of keratin, a protein that also forms the hair and nails. Cutaneous horns may be benign, precancerous, or cancerous.
About 40%Trusted Source of all cutaneous horns are malignant, and the most common associated skin cancer is squamous cell carcinoma.
For this reason, anyone who may have cutaneous horns should contact a doctor for a biopsy to determine whether the growth is cancerous.
After the doctor removes the growth, most people do not need further treatment, though they may need regular screening to determine whether the cancer has returned.
1000-Lb. Sisters’ Tammy Slaton Barely Recognizable After Showing Off Skin Removal Surgery Results
Tammy Slaton is showing off her new figure after undergoing skin removal surgery.
The 1000-Lb. Sisters star posted a series of photos on TikTok that show the 38-year-old smiling while posing in black, body-hugging shapewear and holding up a peace sign in a yellow tank top and pair of jeans.
Tammy underwent her skin removal surgery on January 18, and the results were recently revealed on her reality show.
Highlights
Tammy Slaton revealed dramatic results after an 8-hour skin surgery removing over 15 lbs. of excess skin.
She lost more than 500 lbs., transforming her health and mobility.
Tammy shared her transformation on TikTok, showing confidence and a new slimmed-down look.
During the 8-hour procedure, doctors removed “over 15 lbs.” (approx. 6 kg) of excess skin from her chin, stomach, and arms, which had been left hanging after her impressive 500-pound weight loss.
Tammy Slaton stunned with her new look after undergoing skin removal surgery
Before the operation, Tammy, who stars on 1000-Lb. Sisters alongside her sister Amy Slaton-Halterman, opened up about the excitement she felt upon receiving the green light from her doctors, as well as the nerves she had about the complex procedure.
“After six years and losing over 500 pounds, I was finally approved for surgery,” she told People last month.
“I was just overwhelmed with excitement. I worked really hard for this, and now it’s here. I’m pretty sure it was noticeable on my face how immediately shocked and then overwhelmed with joy I was.”
Tammy stars with her sister Amy on the TLC reality show 1000-Lb. Sisters
Tammy continued: “I was really nervous for the skin removal surgery because I was really just kind of afraid of how I’m gonna feel looking at myself without the belly there.
“The night before my surgery, I was seriously freaking terrified.”
The reality star revealed that she was more nervous about the skin removal surgery than she was about getting bariatric surgery in 2022.
Tammy’s siblings Amy, Amanda, Misty, and Chris were waiting for her when she returned to her Pittsburgh home from the surgery and praised her dedication to improving her health throughout her lengthy weight-loss journey.
“Oh my God, she looks great,” Misty said on the show. “When she started, she weighed 730 lbs. (330 kg) and we couldn’t even get her to walk to the mailbox. Now she’s lost 500 lbs (226 kg). I mean, that’s a couple people, not just one person! I am so proud of her, it’s just unreal.”
Since starting her weight-loss journey, she has shed over 500 pounds (226 kg)
Tammy told People that doctors were “surprised” with how well her body was healing and that she was able to return home four days earlier than expected.
After her weight loss, her surgeon recommended skin removal surgery because her loose skin was affecting her mobility
The 38-year-old, who announced her engagement to fiancée Andrea Dalton in June, shared a series of selfies reflecting her transformation in a July 1 TikTok.
“So much [has] changed about me over the years,” she captioned the post. “I couldn’t be more thankful and blessed to have the support and love not only from my fans/besties but my girlfriend and ofc my family.”
Tammy has starred on the TLC reality show 1000-Lb. Sisters with her sister Amy since 2020. The show chronicles the sisters’ daily lives and efforts to lose weight.
Thanks to her weight-loss transformation, the Kentucky native no longer needs a walker or the oxygen support tank she had used for 15 years.
Her bariatric surgeon, Dr. Eric Smith, explained on the show that Tammy’s loose skin had to be removed to improve her quality of life.
“Generally, we want patients to have achieved the majority of their weight loss and maintained a stable weight for 3-6 months before proceeding with skin removal,” he said.
“However, in Tammy’s case, she has a significant amount of loose skin that’s affecting her mobility and contributing to other health concerns. Given this, it makes sense to consider surgery sooner rather than later, even though she will continue to lose weight in the future.”
The surgeon added: “There was a period when she didn’t feel worthy of feeling better or living a healthier life. Helping her recognize her self-worth has been just as rewarding as seeing the weight come off. It’s been a key factor in her success.”
Between 2020 and 2022, Tammy lost 200 pounds (90 kg) after her doctor informed her that she needed to lose weight in order to qualify for bariatric surgery. A year after the procedure, she lost another 300 pounds (136 kg).
The reality star underwent bariatric surgery in 2022 and lost 300 pounds (136 kg) the following year
In November 2024, the reality show captured the emotional moment when she stepped on a scale and learned she weighed 281.2 pounds (127 kg).
“I think the last time I weighed 281 [pounds], I was in fourth or fifth grade,” she said.
Netizens congratulated the 38-year-old on her remarkable transformation
When a stroke is a stroke mimic? | Hillcrest Medical Center in Tulsa, Oklahoma
10 Warning Signs of Stroke One Month Before – Unbelievable Signs… Revealed
Scroll to the bottom for a quick read, all the 10 warning signs briefly written there.
Well hello there, friend. It’s so good to have you here today. Tell me, have you ever woken up feeling just a little “off”? Maybe you noticed your coffee cup trembling in your hand, or you felt a sudden wave of dizziness while watering the plants? You brushed it off—thought it was just fatigue or a touch of arthritis acting up. I’ve been there too. But what if I told you those little moments might be whispering something important? Something we absolutely need to listen to?
You see, as we get a little wiser in our years—60, 70, and beyond—our bodies sometimes send us signals. Quiet warnings that, if we catch them early, could change everything. Today, I want to talk about one of the most important conversations we can have: the subtle signs that a stroke might be on the horizon. And here’s what’s surprising—these signs can appear weeks before, even a full month. Catching them? That’s our superpower.
Stroke Warning Signs for Seniors Discussed as Stroke has changed his face
Now, I know the word “stroke” can feel heavy. But think of this as sitting down with a dear friend over tea, sharing what we’ve learned to keep each other safe. Together, we’ll walk through 10 quiet warnings our bodies might give us. Today, we’ll start with the first three. And I promise—no complicated medical jargon, just straight-from-the-heart talk. Because you deserve to feel empowered, not overwhelmed.
Let’s begin with one you might not expect. It’s not the classic “face drooping” you hear about in emergencies. No, this one’s quieter. Have you ever had a headache that felt… different? Not your usual tension or sinus ache, but something sharper, like a lightning bolt in your head? Or maybe a dull throb that settled in and just wouldn’t leave? My neighbor, Martha—bless her—called it her “angry headache.” She’d never had migraines, but one week, out of nowhere, this pounding started behind her left eye. She took aspirin, rested, but it lingered. A month later, she had a stroke.
Here’s the key: when headaches appear suddenly, feel unusually intense, or seem disconnected from your normal patterns, they can be a red flag. Why? Because strokes often start with changes in blood flow to the brain. Think of it like a river—when the current shifts, it sends ripples upstream first. So if a headache feels “new” or “strange,” please, don’t dismiss it. Tell someone. Call your doctor. Write it down in that little notebook by your phone. It’s not being dramatic—it’s being wise.
Example of how Stroke happens in human heads
Now, let’s talk about something that might seem ordinary: balance. And I don’t mean the “I stood up too fast” wooziness we all know. I mean moments where the room genuinely spins—like you’ve stepped off a merry-go-round. Or maybe you feel strangely anchored to the floor, as if your legs aren’t quite obeying. My friend, this isn’t just “getting older.” It could be your brain struggling to map your place in space.
Picture this: You’re walking to your garden shed, a path you’ve taken for 20 years. Suddenly, you veer sideways, bumping into the roses. Or maybe you reach for a shelf and miss the jar completely. These tiny stumbles can signal that blood flow to the cerebellum—the brain’s balance center—isn’t quite right. And here’s what’s important: it might not last. An hour later, you feel steady again. But that brief wobble? It’s worth paying attention to. So next time it happens, sit down, breathe, and ask yourself: “Is this new?” If it is, treat it like a friendly tap on the shoulder from your body.
Finally, let’s talk about your hands. Have you ever picked up a pen and felt… nothing? Like your fingers were wrapped in cotton? Or woken up with a patch of skin on your arm that felt oddly numb, like it fell asleep? Now, we’ve all had a limb “tingle” after sitting too long. But when numbness or tingling appears without pressure—especially on just one side—and lingers longer than a few minutes? That’s our third sign.
Example of how Stroke happens in human heads
Take my cousin, Frank. He was whittling on his porch last spring when his right hand suddenly felt “cold and heavy.” He thought he’d pinched a nerve. Thirty days later, he had a stroke affecting that same side. Here’s why this happens: your nerves are like a network of tiny wires. When blood flow dips, those wires misfire. So if you notice unexplained numbness in your face, arm, or leg—even if it fades quickly—don’t chalk it up to “sleeping funny.” Tell your doctor. Describe it. Keep track. Because your body’s whispers are kinder than its shouts.
So here’s where we are: First, those new and unusual headaches. Second, balance hiccups that feel out of character. Third, numbness or tingling that shows up uninvited. These aren’t reasons to panic—they’re reasons to pause. To listen. To act.
You know, I think the greatest gift we give ourselves as we age is paying attention. Noticing the quiet things. So next time you feel one of these little signs? Take a breath. Write it down. Share it with someone who cares about you. And remember—we’re just getting started. There’s more to share, and I’ll meet you right back here to continue this conversation. Until then, be kind to that wonderful body of yours. It’s been carrying you through a beautiful, long life—and it’s not done yet.
Brain stroke symptoms cause risk factors diagnosis and treatment – Citycare
Now, let me ask you something: When was the last time your eyes played tricks on you? And I don’t mean needing stronger reading glasses or squinting at small print—that’s just part of the adventure of getting older! I mean moments where your vision changes suddenly. Maybe for a few minutes, the world goes blurry, like you’re looking through frosted glass. Or perhaps you lose a slice of your sight—like a curtain falling over one eye.
My dear friend, Elsie, noticed this last spring. She was deadheading her marigolds when her left eye went dark for nearly ten minutes. “Just tired,” she told herself. But friends, that “tired” was her brain’s way of waving a flag. When blood flow to the optic nerve dips—even briefly—it can dim our vision like a flickering lamp. So if your eyesight does something odd or fleeting? Don’t shrug it off. Note the day, the time. Tell your daughter or neighbor. It’s not fussing—it’s taking the reins.
Next—let’s talk about your brilliant mind. We all forget where we put our keys sometimes (Heaven knows I’ve found mine in the fridge!). But have you ever felt suddenly… lost? Not just forgetful, but genuinely confused in a place you know well? Like standing in your own kitchen, wondering what the kettle is for? Or struggling to form a sentence mid-conversation, as if the words evaporated?
Stroke | The Foundation to Advance Vascular Cures
This happened to my neighbor, Sam. A retired teacher—sharp as a tack!—who suddenly couldn’t recall his grandchild’s name during a video call. For five minutes, his thoughts scattered like leaves in the wind. He blamed stress. But a month later? A stroke. What Sam felt was his brain’s language center briefly “stalling” from reduced blood flow. So if you or a loved one has a sudden “gap” in thinking or speaking—even if it passes—treat it like a check-engine light. Gently say, “Let’s get this looked at.”
Now, here’s a sign we often dismiss as “just aging”: a bone-deep weariness. Not the good kind of tired after gardening or a walk with grandkids—but exhaustion that feels heavy. Like you’ve run a marathon in your sleep. You nap but wake up drained. Your arms feel like lead stirring oatmeal.
Margaret, who joins me for bingo every Tuesday, felt this last winter. “I’m just slowing down,” she’d say. But her “slowdown” was sudden—a profound fatigue that made her breathless climbing stairs she’d tackled for years. Turns out, her heart was struggling to pump blood efficiently to her brain—a quiet red flag. So if your energy plummets without reason—especially alongside other signs we’ve talked about—it’s not “laziness.” It’s your body whispering: “Pay attention here.”
So let’s gather what we’ve shared:
Vision changes that flicker like a candle (blurriness, dark patches, double vision).
Confusion or speech hiccups that feel out of character (lost words, disorientation).
Unexplained exhaustion that weighs you down like a wet coat.
You know, our bodies speak to us in gentle ways long before they shout. These signs? They’re not meant to scare us—they’re invitations. Invitations to pause, to act, to partner with our doctors. And every time you listen, you’re writing a love letter to your own well-being.
We’ve covered six signs now—half our journey. But there’s more to share, and I’ll meet you right here next time to walk through the rest. Until then, keep noticing, keep nurturing that wonderful spirit of yours. And if something feels “off”? Honor that feeling. You’ve earned the right to be your own best advocate.
Understanding Brain Stroke: Symptoms, Causes, and Treatment
Let’s start with something we rarely talk about: swallowing. Now, we’ve all had a sip of tea go down the “wrong pipe” now and then—a little cough and we’re fine. But have you ever felt like food just… sticks? Like your throat forgets how to swallow? Or maybe you’ve choked on something soft—a bite of mashed potato or oatmeal—when you never used to?
My aunt Dorothy noticed this last summer. She’d always loved her morning toast, but suddenly, she’d cough violently after a small bite. She blamed “dry bread” and dunked it in tea. But weeks later, she had a stroke. What Dorothy felt was her brain’s subtle struggle to coordinate muscles in her throat—a sign that blood flow to those nerves might be changing. So if swallowing feels awkward or risky—even once—don’t ignore it. Tell your doctor, “Something felt different.” That simple sentence could change everything.
Next—let’s talk about your smile. Not the one you share with grandkids, but the one you see in the mirror. Have you ever noticed one side of your face feeling… lazy? Like when you try to grin, that corner just doesn’t lift? Or maybe you sip soup and a little dribbles out without you noticing?
Henry, who plays chess at our community center, brushed this off as “Bell’s palsy.” But when his wife saw his smile sag for a full afternoon, she insisted on the ER. Turns out, it was a TIA—a “mini-stroke”—warning of a bigger one coming. The nerves controlling our face are delicate. When blood flow dips, they falter. So tomorrow, when you brush your teeth, smile at the mirror. If one side hesitates, treat it like a friendly tap on the shoulder. Call your nurse or drive to urgent care. Don’t wait for it to “pass.”
Brain Stroke is a Life life-Threatening Ailment that can be Cured if Treated on Time
Now, this one’s subtle but vital: emotions that crash over you like a wave. Have you ever felt suddenly, overwhelmingly sad—for no reason? Or burst into tears watching a commercial you’ve seen a hundred times? Maybe rage flares up over something tiny, like a misplaced remote?
My friend, this isn’t just “having a bad day.” When blood flow shifts in the brain, it can stir our deepest feelings like a spoon in honey. My neighbor, Louise—a cheerful soul—sobbed for an hour because her daisies wilted. She felt embarrassed. But a month later? A stroke. Our brain’s mood centers are sensitive. If your emotions swing wildly or feel alien to you, honor that. Say to someone, “My feelings don’t match my heart today.” It’s not weakness—it’s wisdom.
Finally—let’s talk about your heart’s rhythm. Not the steady beat when you’re resting, but those odd moments when it flutters like a bird in your chest. Or races when you’re just sitting still. Maybe it skips a beat, leaving you breathless.
Arrhythmias—like atrial fibrillation—are silent stroke warnings. Blood pools instead of flowing, forming tiny clots that can travel to the brain. My brother-in-law, Walt, felt his heart “dance” for minutes at a time. He called it “excitement.” But when he finally mentioned it to his doctor? They found a-fib—and prevented a stroke. So if your heart hiccups, flutters, or races—especially with any other sign we’ve shared—grab your phone. Record your pulse. Show your doctor. It’s the greatest gift you can give your future self.
So here we are—all ten whispers:
New, severe headaches
Sudden balance loss
Unexplained numbness
Blurred or lost vision
Confusion or lost words
Crushing fatigue
Trouble swallowing
Facial weakness
Emotional storms
Heart flutters or skips
But here’s what matters most: You are not powerless. When you notice one of these—especially if it’s sudden or paired with another—think “F.A.S.T.”:
Face drooping?
Arm weakness?
Speech trouble?
Time to call emergency services?
Yet even without F.A.S.T., those subtle signs we’ve shared? They’re your early-warning system. Your body saying, “Let’s fix this before it becomes an emergency.”
So today, I invite you: Be kind to yourself. Keep a little journal by your coffee pot. Jot down dates and symptoms. Share it with your doctor like you’d share a grandchild’s milestone—proud you noticed. And if something feels “off”? Dial that number. Walk into that clinic. You’ve spent a lifetime caring for others. Now, let the world care for you.
You are worth it. Every call. Every check-up. Every moment of attention you give yourself.
Thank you for trusting me with your time. Remember: Aging isn’t about slowing down—it’s about waking up. Waking up to the wisdom of our bodies, the strength of our spirits, and the incredible power of paying attention.
Until next time, my friend. Here’s to honoring your strength, your courage, and the gift of time you’ve been given. Take good care.
25 Causes of Raised Skin Bumps ( Pictures & Videos)
Skin conditions like acne, keloids, allergies, and shingles may cause raised skin bumps. Bumps may also occur with more severe health conditions that require medical attention, such as MRSA, cellulitis, or cancer.
Raised skin bumps are very common and harmless in most cases. They may vary in appearance and number depending on the cause.
Skin bumps may be the same color as your skin or a different color. They may be itchy, large, or small. Some can be hard, while others can feel soft and movable.
Most skin bumps do not need treatment. However, it’s important that you speak with a healthcare professional if your bumps are causing discomfort, like burning pain and persistent itching. It’s also recommended that you contact them if you’re concerned about any changes in your bumps or the overall condition of your skin.
Acne
Share on PinterestHealthline/Getty Images
commonly located on the face, neck, shoulders, chest, and upper back
skin breakouts typically blackheads, whiteheads, pimples, or deep, painful cysts and nodules
may leave scars or darken the skin if untreated
Acne is the most common skin condition in the United States, according to the American Academy of Dermatology. It causes skin bumps that can range from very small and painless to large and painful. The bumps are usually accompanied by redness and swelling.
Learn about the types of acne and how to treat them.
Oppenheimer: Watch For Free
Find a girl! 100% Free website!
Contact dermatitis
Share on PinterestTisforThan/Shutterstock
appears a few hours to days after contact with an allergen or irritant
presents a visible rash with borders and appears where your skin came in contact with an irritating substance
itchy, scaly, or raw skin
red in light skin and darker brown, purple, or gray in dark skin.
blisters that weep, ooze, or become crusty
Contact dermatitis is a condition that causes an itchy, red rash when your skin comes in contact with an allergen (like poison ivy) or irritant (like bleach). The rash may consist of raised, red bumps that ooze, drain, or crust.
Learn about contact dermatitis treatments.
Keratosis pilaris
Share on PinterestTai Ketlakorn/Shutterstock
most often seen on the arms and legs but might also occur on the face, buttocks, or torso
patches of skin that appear bumpy, slightly red or discolored, and feel rough to the touch
may get worse in dry weather
Keratosis pilaris is a common skin condition marked by an overgrowth of a protein called keratin. It causes small bumps around hair follicles on the body. The condition often clears up on its own by your mid-20s.
Learn more about how keratosis pilaris may appear on darker skin.
Growths
Bulla
Share on PinterestClément Bucco-Lechat, CC BY-SA 3.0, via Wikimedia Commons
clear, watery, fluid-filled blister that is greater than 1 centimeter (cm) in size
if clear liquid turns milky, there might be an infection
Bullae (plural of bulla) are raised, fluid-filled bumps that can result from friction or conditions like contact dermatitis and chickenpox. They usually go away within a week, but it’s advised that you see a doctor if they become infected or need to be drained.
Learn more about fluid-filled blisters.
Cherry angioma
Share on PinterestRupendra Singh Rawat/Getty Images
can be anywhere on the body but is most common on the torso, arms, legs, and shoulders
small, bright red or purple circular or oval spots that may be raised or flat
may bleed if rubbed or scratched
generally harmless but may require removal if they’re in problem areas
Cherry angiomas are common skin growths that can form in most areas of the body. They develop when blood vessels clump together, creating a raised, bright-red bump under or on the skin. They appear with increasing age, often starting in your 20s or 30sTrusted Source.
Corns and calluses
Share on PinterestVitalis83/Shutterstock
small circles of thickened skin with a painful, horn-like central area of hardened tissue
commonly found on the tops and sides of the toes and on the soles of the feet
also possible in the hands
Corns or calluses are rough, thickened areas of skin caused by friction and pressure. They’re most often found on the feet and hands.
Learn how to get rid of corns at home.
Cyst
Share on PinterestZay Nyi Nyi/Shutterstock
slow-growing bump under the skin that has a smooth surface
can be large or small and is usually painless
typically not a problem unless it’s infected, very large, or growing in a sensitive area
some grow deep inside your body where you can’t see or feel them
Cysts are growths that contain fluid, air, or other substances. They develop under your skin in any part of your body. They feel like a small ball, and you can usually move them around slightly.
Discover how home remedies might help with cysts.
Keloids
Share on PinterestHarold Diaz Lara/Shutterstock
develops at the site of a previous injury
lumpy or rigid area of skin that may be painful or itchy
area is flesh-colored, pink, or red
Keloids are smooth, raised growths that form around scars. They’re most commonly found on the chest, shoulders, and cheeks. They’re similar to hypertrophic scars but can grow to be much larger than the original wound.
Learn how to help reduce the appearance of keloids.
Lipoma
Share on PinterestCasa nayafana/Shutterstock
soft to the touch and moves easily if prodded with your finger
small, just under the skin, and pale or colorless
commonly located in the neck, back, or shoulders
only painful if it presses on a nerve
Lipomas are collections of fatty tissue under the skin and are often painless. They usually form on the neck, back, or shoulders. They’re typically harmless, but you can remove them for cosmetic reasons or if they cause pain.
Learn more about lipoma removal surgery.
Nodule
Share on PinterestPhoto by DermNet New Zealand
small to medium growth that may be filled with tissue, fluid, or both
usually wider than a pimple and may look like a firm, smooth elevation under the skin
usually harmless but may cause discomfort if it presses on other structures
may also be located deep inside the body where you can’t see or feel them
Nodules result from abnormal tissue growth. They appear in common areas like the armpits, groin, and head and neck region.
Seborrheic keratosis
Share on PinterestSutedja, E. K., Ahmed, R., Sutedja, E., Rowawi, R., Suwarsa, O., & Gunawan, H. (2021). A Successful Defect Closure After Total Excision of Seborrheic Keratoses with Atypical Clinical Presentation Using Island Pedicle Flap in an Elderly Patient. International medical case reports journal, 14, 157161
round, oval, dark-colored growth with a “stuck-on” appearance
can be located anywhere on the body except for the palms of the hands and soles of the feet
raised and bumpy with a waxy feel
may be skin-colored, brown, or black
Seborrheic keratoses (plural of keratosis) are common, harmless skin growths usually seen in older adults. They appear as round, rough spots on the surface of the skin. They can affect many areas of the body, including the chest, shoulders, and back.
Learn how to tell the difference between seborrheic keratosis and melanoma.
Skin tags
Share on PinterestVitalis83/Shutterstock
skin growths that can become up to a half-inch long
same color as your skin or slightly darker
most likely friction-related cause
commonly found near the neck, armpits, breasts, groin, stomach, or eyelids
Skin tags are small, fleshy flaps of skin. They usually grow on the neck or in the armpits. They may be the same color as the skin or slightly darker.
Review the differences between moles and skin tags.
Strawberry nevus
Share on PinterestGstk, CC BY-SA 4.0, via Wikimedia Commons
red or purplish raised mark, commonly located on the face, scalp, back, or chest
appears at birth or in very young children
gradually gets smaller or disappears as the child ages
Strawberry nevus is a red birthmark also known as a hemangioma. They are most common in young children and usually disappear by age 10 years.
Infections
Certain bacterial and viral infections cause skin bumps. Some may go away on their own and may not require treatment. But some will only get worse if they go undiagnosed and untreated.
Boils
Share on PinterestTejas Prajapati/Shutterstock
bacterial or fungal infection of a hair follicle or oil gland
can appear anywhere on the body but are most common on the face, neck, armpit, and buttock
red, painful, raised bump with a yellow or white center
may rupture and weep fluid
Boils (aka furuncles) are infected hair follicles that look like red, raised bumps on the skin. They can be painful but eventually go away once they burst and release fluid.
Learn whether you should pop a boil on your own.
Chickenpox
Share on PinterestMixmike/Getty Images
clusters of itchy, red, fluid-filled blisters in various stages of healing all over the body
accompanied by fever, body aches, sore throat, and loss of appetite
remains contagious until all blisters have crusted over
Chickenpox is a common childhood virus characterized by red, itchy bumps that form all over the body. Adults can get it too, and symptoms are often more severe.
Learn about the varicella vaccine to help protect yourself against chickenpox.
Cold sore
Share on PinterestKuzenkova_Yuliya/Getty Images
red, painful, fluid-filled blister that appears near the mouth and lips
affected area will often tingle or burn before the sore is visible
may be accompanied by mild, flu-like symptoms, such as low fever, body aches, and swollen lymph nodes
Cold sores result from activation of the herpes simplex virus. They appear as red, fluid-filled blisters around your mouth and other areas of your face. They’re most contagious when they burst open but still contagious when they’ve scabbed over.
Learn more about what can trigger the virus that causes cold sores.
Impetigo
Share on PinterestZay Nyi Nyi/Shutterstock
common in babies and children
irritating rash and fluid-filled blisters that pop easily and form a honey-colored crust
rash is often located in the area around the mouth, chin, and nose
Impetigo is a highly contagious bacterial skin infection common in young children. Adults with impetigo often contract the infection from skin-to-skin contact as part of contact sportsTrusted Source.
Discover natural home remedies for impetigo.
Molluscum contagiosum
Share on PinterestMediscan / Alamy Stock Photo
bumps that may appear in a patch of up to 20
small, shiny, and smooth
flesh-colored, white, or pink
firm and dome-shaped with a dent or dimple in the middle
Molluscum contagiosum is a typically harmless viral infection that can affect all parts of your body. These small, flesh-colored bumps can arise from skin-to-skin contact with someone with the infection. It’s most common in children ages 2–5 yearsTrusted Source, but adults can get it too.
Learn how molluscum contagiosum is passed on and how to prevent it.
MRSA (staph) infection
Share on PinterestKey West Wedding Photography – Cayobo
skin infection that often looks like a spider bite, with a painful, raised, red bump that may drain pus
needs to be treated with powerful antibiotics and can lead to more dangerous conditions like cellulitis or blood infection
An MRSA (staph) infection is triggered by a type of Staphylococcus, or staph, bacteria resistant to many different antibiotics. These bacteria commonly live on the skin but can cause an infection when they enter through a cut or scrape.
Learn what to expect as your staph infection heals.
Scabies
Share on PinterestPublic domain, via Wikimedia Commons
symptoms may take 4–6 weeks to appear
extremely itchy rash that may be pimply, made up of tiny blisters, or scaly
raised white or flesh-colored lines
Scabies is a skin infestation of a tiny mite called Sarcoptes scabiei. It produces an itchy, pimple-like rash. Without treatment, they can live on your skin for up to 2 monthsTrusted Source.
Discover home remedies for scabies.
Wart
Share on PinterestmuroPhotographer/Shutterstock
may be found on the skin or mucous membranes
may occur as one wart or in groups
may be skin-colored, pink, or slightly brown
Warts are raised, rough bumps caused by the human papillomavirus (HPV). They typically develop on the hands and feet, but it’s important to see a doctor if they develop on your face or other sensitive areas. They’re also contagious and can cause you to pass HPV to others.
Discover home remedies for warts.
Skin cancer
Skin cancer can cause other types of raised skin bumps. There are several types of skin cancer, all requiring medical management and treatment.
Actinic keratosis
Share on PinterestJodiJacobson/Getty Images
typically less than 2 cm, or about the size of a pencil eraser
thick, scaly, or crusty skin patch that may itch or burn
appears on parts of the body that receive a lot of sun exposure (hands, arms, face, scalp, and neck)
usually pink in color but can have a brown, tan, or gray base
Actinic keratosis is a precancerous skin condition usually due to sun exposure over a long time. It’s more common in older adults and people with lighter-colored skin.
Learn more about the differences between actinic and seborrheic keratosis.
raised, firm, and pale areas that may resemble a scar
dome-like, shiny, and pearly areas that may have a sunk-in center, like a crater
may be pink, red, or discolored
visible blood vessels on the growth
easy bleeding or oozing wound that does not seem to heal or heals and then reappears
Basal cell carcinoma affects the cells in the lower layer of your epidermis. It produces painful bumps that bleed in the early stages. It’s the most commonTrusted Source form of skin cancer and has a very high survival rate.
Learn more about Mohs surgery, a standard treatment for basal cell carcinoma.
often occurs in the face, ears, and back of the hands
scaly, reddish patch of skin that progresses to a raised bump and continues to grow
growth that bleeds easily and does not heal, or heals and then reappears
Squamous cell carcinoma begins in the squamous cells in the outermost layer of your skin. The condition causes scaly, red patches and raised sores to develop on the skin. These abnormal growths often form in areas exposed to ultraviolet (UV) radiation.
Learn more about the different types of nonmelanoma skin cancer.
Melanoma
Share on PinterestNasekomoe/Shutterstock
mole anywhere on the body that has irregularly shaped edges, asymmetrical shape, and multiple colors
mole that has changed color or gotten bigger over time
usually larger than a pencil eraser
Melanoma is the least common but most serious form of skin cancer. It begins as an atypical mole. Cancerous moles are often asymmetrical, multicolored, and large, with irregular borders. They can appear anywhere on the body.
View more pictures of melanoma.
Other causes of skin bumps
Allergic reactions to foods, pollen, and dust mites, among others, may cause skin bumps called hives. Hives can be the same color as your skin or appear slightly red or discolored. They may be small or large, and they’re usually itchy and develop in clusters.
Ringworm may also cause a raised ring-shaped rash. It is caused by a fungus and requires medical treatment.
Cellulitis is another option. It causes a discolored, swollen rash that is painful and spreads. It is caused by a bacterial infection and is considered a medical emergency.
When to see a doctor about raised skin bumps
Most skin bumps are harmless and aren’t cause for concern. However, it’s important that you see a doctor if you:
have skin bumps that last for a long time
experience pain or high discomfort
don’t know the cause of the bumps
notice a growth that changes in color, shape, or size
have oozing or bleeding lesions
A healthcare professional will perform a physical examination and inspect the skin bumps. Expect to answer questions about your bumps, medical history, and lifestyle habits.
A doctor may also perform a skin biopsy to test if the skin bump is cancerous. This procedure involves taking a small sample of skin tissue from the affected area for analysis. Depending on the results, the doctor may refer you to a dermatologist or other specialist for further evaluation.
Treatment for raised skin bumps
Removal
Treatment for raised skin bumps depends on the underlying cause. Most common causes of skin bumps are harmless, so you probably won’t need treatment. However, if your skin bumps are bothering you, you might be able to have them removed for cosmetic reasons.
For example, a dermatologist can remove skin tags or warts by freezing them off. They can also surgically remove certain skin bumps, including cysts and lipomas.
You might be able to remove some itchy or irritating bumps with topical ointments and creams.
If a doctor finds that your skin bumps are cancerous or precancerous, they will most likely remove the bumps completely. You will also need to attend regular follow-up appointments so your doctor can check the area and make sure the cancer does not come back.
Medication
In cases where additional medical treatment is required, a doctor will prescribe medications that can help eliminate your skin bumps and the underlying cause.
For a bacterial infection, such as MRSA, you may need antibiotics. For a viral infection, such as chickenpox, a doctor may recommend over-the-counter medications and home treatments.
Some viral infections, such as herpes, cannot be cured. However, a doctor can give you medications to help ease symptoms.
Takeaway
Most skin bumps are due to harmless, temporary conditions that don’t require treatment. If your skin bumps are due to an infection or long-term condition, timely medical treatment usually helps clear them up or ease symptoms.
If your skin bump is cancerous, your outlook is improved if healthcare professionals detect and treat cancer early.
Woman who spent £13,000 to have her ribs removed says people keep asking if she is ‘going to eat them.’
No, she’s not going to eat her own ribs just because you ask her to
A woman who had six of her ribs removed has got plans for what to do with them, and it’s not what people keep asking her.
Emily James lives in Kansas City, US, which you’d think would be based in Kansas but is actually just across the state border in Missouri, even though it has a suburb called Kansas City, which actually is in Kansas.
However, we’re not here to talk about where she lives but what she’s going to do with her ribs.
The 27-year-old went in for some cosmetic surgery costing $17,000 (£13,568) so she could have a smaller waist and also got a breast augmentation done.
After the surgery, they let her keep her own ribs, and people have had all sorts of suggestions as to what she ought to do with them.
Emily James had six of her ribs removed (EMILY JAMES / CATERS NEWS)
Some people have suggested she make adult toys out of the bones, while others have asked if she’d consider resorting to cannibalism and eating her own spare ribs.
Emily was originally planning on gifting the ribs to a friend, but has instead come up with another idea of what to do with the extra bits of ribcage she no longer needs.
“I plan on having someone make a crown out of them. “They let me keep the ribs and I was initially going to gift them to my best friend,” she said of her big idea of what to do with the surgically removed bones. She also shot down the suggestions that she engaged in cannibalism with her own removed body parts.
“I plan on making them into a crown. I’ve had people say they would make them into a chew toy or boil them down into broth,” she said.
“Personally, I think my meat would taste delicious. Eating human meat can cause a plethora of disorders that are fatal. So, I will not be partaking in cannibalism, thank you.”
It turns out you can’t just get six of your ribs (three from each side, naturally) removed without some discomfort, as Emily has had to wear a corset constantly to deal with the swelling.
However, despite this, she says she’d only rate the pain she feels as two out of 10 thanks to the team of doctors and nurses helping her recover from her surgery.
There have been some critics, but Emily said in a video that ‘getting my ribs removed doesn’t change the fact that I’m a kind, loving trans girl.’.
She said, “I know some of your moms walk around with BBLS; how is this any different?
“It is my money, my body, and I’m going to do what I want with it.”
Did you know that something as simple as an onion could play a role in keeping your lungs healthy? While onions are a staple in kitchens around the world, their health benefits extend far beyond their culinary uses. This article explores the connection between onions and lung health, shedding light on their potential to improve respiratory wellness.
Onions: A Natural Source of Health Boosters
Buy vitamins and supplements
Onions are packed with powerful nutrients, including antioxidants, vitamins, and natural compounds like quercetin. These components are known to fight inflammation and boost the immune system. Quercetin, in particular, has been studied for its ability to reduce oxidative stress and improve lung function, making it a valuable ally in preventing respiratory diseases.
Lung Health and the Power of Detoxification
The lungs are constantly exposed to harmful particles from air pollution, cigarette smoke, and environmental toxins. Over time, these elements can compromise lung function. Onions, with their sulfur-rich compounds, act as natural detoxifiers, helping to clear mucus and toxins from the respiratory tract. This not only supports lung health but also enhances oxygen absorption and circulation.
How to Incorporate Onions Into Your Diet
Incorporating onions into your daily meals can be incredibly simple and rewarding. Here are some tips:
Add thin slices of raw onion to your salads for a crunchy, tangy twist.
Use onions as a base for soups, stews, and stir-fries to maximize their flavor and health benefits.
Roast onions with a drizzle of olive oil for a sweet, caramelized treat that pairs well with almost any dish.
Beyond Nutrition: Onions in Traditional Remedies
For centuries, onions have been used in traditional remedies to treat respiratory conditions. A popular home remedy involves boiling onion slices with honey to create a soothing syrup for coughs and colds. While these remedies aren’t substitutes for medical treatment, they highlight the potential of onions as natural lung supporters.
Take a Deep Breath With Confidence
While onions alone can’t replace a healthy lifestyle, they can complement your efforts to maintain optimal lung health. Combined with regular exercise, a balanced diet, and avoiding pollutants, onions can serve as a simple yet effective tool in protecting your respiratory system.
Conclusion
The humble onion is more than just a flavorful ingredient—it’s a natural ally for your lungs. By understanding its benefits and incorporating it into your diet, you can take proactive steps toward better respiratory health. So, the next time you’re preparing a meal, think about the powerful impact a single onion can have on your overall wellness.
It’s the morning of your big event and you are greeted with a pimple. Ugh. Why do pimples always have such poor timing? You may be tempted to pop this unwanted guest, but it’s not a good idea. Contrary to what pimple popping videos may show, squeezing your skin to extract the contents of a pimple — a mixture of oil, dead skin and bacteria — can cause scarring and infection. It can also worsen inflammation, making the pimple larger, more red and more painful.
A Pimple Primer
Any manipulation with popping a pimple can cause lasting color or pigment change.
— Lauren Taglia, MD, PhD
When your pores get clogged, a few types of pimples may emerge. The most common types of pimples are:
Whiteheads: These closed comedones have a white, pus-filled top and stay closed on the surface of your skin.
Blackheads. These open comedoneshave a small, black opening at the top. The black coloring is not from dirt, but rather from the process of oxidation. The oil and dead skin from your clogged hair follicle has been exposed to air.
Papules: These inflamed comedones appear as small, pink bumps can be painful.
Pustules: These havepus on the top and a ring of red on the bottom. They look like whiteheads but have the bonus feature of redness around the base.
Cysts: These are pus-filled, deep, painful pimples that can leave scars.
Nodules: Theseare similar to cysts, buthave less fluid, so they are harder. Inflammation in nodules tends to be deep, making them more painful and prone to leaving scars.
Is There One Type of Pimple You Can Pop?
“Not really”, says Lauren Taglia, MD, PhD, a dermatologist at Northwestern Medicine. “But if you must pop, wait until the pimple has been around a few days and has developed a white head, indicating there is pus near the surface. Avoid popping new pimples or those that are red or sore,” she advises.
When doing this at home, many people choose to pop pimples with a lancet needle or pin. This is not a good idea because it can cause an infection if the needle or pin hasn’t been properly sterilized. Additionally, you might penetrate other parts of your skin, causing additional damage. “Any manipulation when popping a pimple can cause lasting color or pigment changes, which may be more frustrating than the initial pimple,” explains Dr. Taglia.
A gentler approach is to use a warm wash cloth or compress. This softens the pimple and helps it form a complete head, which makes it easier to remove. Apply gentle pressure to remove the pus, then apply ice to reduce inflammation.
Do Pimple Patches Work?
The small adhesive disks called pimple patches, acne patches and zit stickers, are designed to cover and protect pimples. They work in several ways:
Absorption: They absorb excess sebum and pus from the pimple.
Protection: They shield the pimple from bacteria and dirt, reducing the risk of infection.
Healing: Some patches contain ingredients that promote healing and reduce inflammation.
Many of these spot treatments are designed to target a pimple with an active ingredient. Common ingredients include:
Hydrocolloid: This polymer forms a gel when mixed with water and is the primary ingredient in most pimple patches. It creates a moist environment that softens the pimple, allowing it to heal faster. This water-attracting substance also draws fluid from the pimple.
Salicylic acid: This beta-hydroxy acid causes the top layer of your skin (epidermis) to slough off, which helps unclog pores, reduce inflammation and support new cell growth.
Tea tree oil: Also known as melaleuca oil, tea tree oil is a natural ingredient that comes from the leaves of the Australian tea tree. This highly concentrated essential oil extract is believed to have antibacterial and anti-inflammatory properties.
Niacinamide: This vitamin B3 derivative helps reduce redness and inflammation.
Pimple patches can be helpful for certain types of acne lesions. “Pimple patches can help absorb drainage and prevent the area from further irritation or trauma. They work best on an open or recently healing papule, pustule or cyst,” says Dr. Taglia.
However, Dr. Taglia notes that pimple patches have some limitations:
They do not work effectively on whiteheads or blackheads.
They are not effective for deeper acne lesions, such as nodules or cysts.
While pimple patches can aid in the healing of existing lesions, they do not actually prevent new acne breakouts from forming.
If pimples become a recurring issue for you, seek the advice of a dermatologist. “There are options for treating an acute pimple, which can speed healing time, as well as longer-term strategies to prevent further breakouts,” says Dr. Taglia.
As the world’s population of adults greater than 60 years old continues to increase, it is important to manage nail disorders that may impact their daily lives. Nail disorders may have significant impact on quality of life due to decreased functionality, extreme pain, or social embarrassment. In this review, we discuss nail disorders affecting older patients, including physiologic, traumatic, drug-induced, infectious, environmental, inflammatory, and neoplastic conditions. Diagnosis of these conditions involves a detailed history, physical examination of all 20 nails, and depending on the condition, a nail clipping or biopsy and/or diagnostic imaging. Nails grow even more slowly in older adults compared to younger individuals, and therefore it is important for accurate diagnosis, and avoidance of inappropriate management and delay of treatment. Increased awareness of nail pathologies may help recognition and management of nail conditions in older adults.
KEY MESSAGES
Nail disorders are common amongst older adults and may cause decreased functionality, pain, psychosocial problems and impact quality of life.
Many nail conditions, both physiologic or pathologic, may have similar presentation in older adults. Confirmation testing is important to avoid inappropriate or delayed treatment.
The increased frequency of comorbidities, drug interactions, polypharmacy, and mental or physical limitations with aging must be considered when managing care of older patients with nail disorders.
Keywords:
Nail disorders
older adults
age
senile
geriatric nail conditions
Previous articleView issue table of contentsNext article
Introduction
The population of adults ages 60 years old is estimated to double to 2.1 billion, and 80 years and older is expected to triple to 426 million by 2050 [Citation1], highlighting the need to diagnose and treat nail disorders that affect the daily lives of older adults in terms of functionality, pain, or social embarrassment. Moreover, more generally dermatologists serve an important role in helping patient navigate the process of healthy aging as they address factors that fundamentally affect both physiologic and pathological processes faced by older adults [Citation2]. In this review, we aim to discuss a breadth of nail disorders affecting older patients , including physiologic, traumatic, drug-induced, infectious, environmental, inflammatory, and neoplastic nail changes.
Table 1. Summary of common nail changes in older adults.
Download CSVDisplay Table
Physiologic changes
Physiologic nail changes in older adults include alterations in color, thickness, contour, texture, growth rate, and chemical composition, which may be due to decreased circulation and changes in elastic or connective tissue [Citation3,Citation4].
Nails of older adults often appear dull, opaque, or pale with white (leukonychia), yellow, brown, or gray discoloration [Citation5]. One type of physiologic leukonychia is Neapolitan nails, which resemble Neapolitan ice cream with a proximal white band and absent lunula, central pink band, and distal opaque band [Citation3,Citation5–7]. The bands remain stable with longitudinal nail growth. In a study of 258 patients >70 years old, 19% of patients had Neapolitan nails, which were associated with osteoporosis and thin skin (p < 0.05) [Citation7].
Nail thickness is variable in older adults, with some presenting with an increase, decrease, or no change in nail thickness. While nails are normally smooth, texture changes associated with aging include increased longitudinal striations that are either superficial (onychorrhexis) or deep (ridging). Onychorrhexis is due to decreased nail matrix cell turnover rate. Other texture changes include transverse grooves, pitting, or trachyonychia (sand paper nails) [Citation3].
The nail contour of older patients has decreased longitudinal convexity with increased transverse curvature [Citation3–6]. Other changes, though not necessarily physiologic changes, include koilonychia (spooning), nail plate flattening, and pincer nails () [Citation3].
Figure 1. Pincer nail of the left first toenail in an 80-year-old woman. The lateral aspect of the nail plate is penetrating the periungual dermis of the lateral nail fold [Citation8].
On average, toenails grow 1.0 mm/month and fingernails 3.0 mm/month. In a study of linear nail growth rate in 192 females and 79 males from 10–100 years old, nail growth decreased by 0.5% per year from 25–100 years old. The thumbnail decreased by 38% between the third and ninth decades. On average, males have faster growth rate until the sixth decade of life, but by the eighth decade females have faster growth rate [Citation9].
Alterations to the chemical composition in nails of older adults include increased calcium and decreased iron [Citation3]. Moreover, there is an increase in collagen cross-linking with aging, which may affect nail flexibility [Citation10]. On histopathology, keratinocytes are larger and there is a greater number of keratinocyte nuclei remnants (pertinax bodies) [Citation3,Citation5]. The nail bed dermis demonstrates blood vessel thickening and degeneration of elastic tissue [Citation3].
Traumatic changes
Onychogryphosis
Onychogryphosis is defined as thickening, hypertrophy, and brown opaque nail plate discoloration, most frequently affecting the great toenails [Citation4,Citation5,Citation11]. It is a frequent problem in older patients, especially in those that are unable to maintain regular nail care. In a cross-sectional observational study of 173 patients (mean age at long term health facility: 85.0 ± 9.7 years, at special nursing home 1: 86.8 ± 7.2 years, and at special nursing home 2: 87.5 ± 7.1 years), prevalence of onychogryphosis was 17.9% [Citation12]. The nail presents as ‘ram’s horn-like’ or ‘oyster-like’ with transverse striations, often associated with trauma, nail surgery, foot-to-shoe incompatibility, or hallux valgus [Citation3,Citation5,Citation11]. Often the nails grow upward and laterally and the direction of growth can be directed by shoe pressure [Citation3,Citation5]. It is frequently associated with poor peripheral circulation (i.e. varicose veins, stasis dermatitis, and lower leg ulcers) [Citation11]. Onychogryphosis can be distinguished from retronychia and onychomycosis by its spiral striations [Citation13] (). Prevention can be achieved with regular nail trimming and wearing comfortable shoes to relieve pressure and limit microtrauma. However, many older adults may be unable to maintain regular nail care, as they may have difficulty trimming their toenails due to mobility limitations [Citation14]. Those who do not have access to help may develop the ‘long toenail sign,’ a potential indicator of difficulties with self-care [Citation14]. Management includes electric filing and drilling for mechanical debridement, chemical nail avulsion via 40% urea or 50% potassium iodide under occlusion, or surgical avulsion with or without matriectomy [Citation11]. After onychogryphosis treatment, patients may see normal nail growth or possible recurrences. Hence treatment may need to be repeated and nails should be kept short to prevent recurrence.
Figure 2. A 75-year-old female presented with painful bilateral great toenails for 10 years. Her nails grew slowly and were extremely difficult to clip. A full nail examination was significant for opaque yellow-brown thickening, hyperkeratosis, elongation, and increased curvature of the great toenails. Onychogryphosis can be differentiated from retronychia and onychomycosis by its spiral striated appearance [Citation13].
Onychocryptosis
Onychocryptosis, or ingrown toenail, presents with pain at rest, ambulation, or with pressure [Citation5]. It has a bimodal presentation, presenting between the first and third decades and then in older adults [Citation8]. It may be caused by trauma, weight fluctuation, hyperhidrosis, poor nail cutting, onychotillomania, history of nail surgery, obesity, bony abnormalities, onychomycosis, foot-to-shoe incompatibility, or hallux valgus [Citation5,Citation8]. With trauma, constricting footwear, or expanding feet secondary to edema or weight gain, a nail barb or spicule can penetrate the nail fold as the nail plate grows [Citation8]. For older patients with comorbidities that result in decreased sensation of feet/toes (i.e. diabetes mellitus, peripheral vascular disease, or arteriosclerosis), patients experience minimal pain and may present with infection, osteomyelitis, or gangrene [Citation5,Citation8]. Prevention can be achieved with regular nail trimming such that the nail plate is cut straight and the corners are beyond the distal edge of the lateral nail folds [Citation8].
Treatment includes conservative approaches, such as taping, cotton packing, dental flossing, nail bracing (orthonyx technique), and super-elastic wiring. If conservative approaches fail, surgical approaches include partial/complete nail avulsion with or without matricectomy [Citation5,Citation8,Citation15]. A systematic review of 18 studies that discussed patient-reported outcomes of onychocryptosis treatments demonstrated that patients receiving both nonsurgical and surgical interventions reported relatively high levels of patient satisfaction [Citation16].
Onychauxis
Onychauxis, or pachyonychia, is defined as localized nail plate hypertrophy with hyperkeratosis, discoloration, and decreased translucency with or without subungual hyperkeratosis and debris [Citation3,Citation5,Citation6]. It may be due to overlapping/underlapping toes, foot-to-shoe incompatibility, digiti flexi, hallux rigidus, or hallux valgus [Citation5], and may result in onycholysis, pain, and increased risk of onychomycosis [Citation3]. Since onychauxis is sometimes misdiagnosed as onychomycosis and inappropriately treated with antifungals [Citation5], confirmatory testing should be performed. Prevention can be achieved with regular nail trimming, while management includes electric filing, chemical nail avulsion via 40% urea, or surgical avulsion with or without matricectomy [Citation3,Citation5].
Onychophosis
Onychophosis is defined hyperkeratosis of the lateral or proximal nail folds, between the nail fold and nail plate, or subungual area. It is common in older patients and the great and fifth toenails are most commonly affected, likely because they are most often subject to trauma. Risk factors include foot-to-shoe incompatibility, digiti flexi, hallux valgus, and rotated fifth toes. Preventative measures include wearing comfortable shoes and relieving pressure. Treatment includes nail debridement or application of keratolytics (i.e. urea 20%, ammonium lactate 12% or salicylic acid 6–20%) [Citation3,Citation5].
Onychoclavus
Onychoclavus, a subungual heloma or corn, presents as hyperkeratosis with or without melanonychia overlying the nail bed typically affecting the distal great toenail [Citation3,Citation5]. It may be resemble benign melanocytic activation or malignant melanoma [Citation4]. Onychoclavus may be due to trauma, foot-to-shoe incompatibility, digits flexi, hallux valgus, hammer toe deformity, or rotated fifth toes [Citation5,Citation6]. Since it is associated with subungual exostosis or chondroma, radiologic examination may be used to rule out an underlying bony abnormality [Citation5]. Management includes avoiding tight-fitting shoes and wearing protective pads to relieve pressure, removal of hyperkeratotic tissue, and surgical correction of any osseous anomaly [Citation3,Citation5,Citation6].
Subungual hematoma and Splinter hemorrhages
Subungual hematomas are common in older patients and initially present as violaceous-black nail plate discoloration that migrates distally with nail growth. Sometimes, onycholysis and nail plate separation ensue [Citation5,Citation17]. Splinter hemorrhages due to trauma in the older adults are most often black and found in the central or distal third of the nail plate [Citation6]. Splinter hemorrhages may also be a sign of nail psoriasis. In a study of 220 patients >65 years, 35 subjects (16%) had splinter hemorrhages [Citation5].
The most common cause of subungual hematoma is trauma, but also may be due to foot-to-shoe incompatibility, hallux rigidus, hallux valgus, or overlapping toes [Citation5]. In older patients, subungual hematomas/splinter hemorrhages may also be due to anticoagulant therapy [Citation6]. A nail clipping with histopathological examination can confirm subungual hematoma. Diagnosis may also be confirmed via serial photography [Citation17] ().
Figure 3. Example of a patient-initiated nail hematoma selfie of the right thumbnail on the day of examination.
Patient-initiated nail hematoma selfie of the right thumbnail 1 month following the initial examination.
Patient-initiated nail hematoma selfie of the right thumbnail 2 months following the initial examination 18.
Treatment includes reassurance and observation of the nail over time to ensure the hemorrhage resolves and moves distally, assuring patients that their nail discoloration is due to blood as opposed to nail melanoma [Citation18]. In acute cases, trephination or complete removal of the nail plate to relieve pressure might help symptomatically when >50% of the nail plate is involved or >25% with fracture [Citation19].
Beau’s lines, onychomadesis and retronychia
Beau’s lines, onychomadesis, and retronychia are hypothesized to lie on a spectrum with a common pathophysiology of an insult to the nail matrix, with slowing or stopping of nail plate production (). Beau’s lines are transverse grooves in the nail plate caused by a temporary decrease of mitotic activity of nail matrix keratinocytes [Citation20,Citation21]. Beau’s lines may be due to trauma, medications, or systemic illnesses [Citation22]. When they present unilaterally, they may be caused by injury to the ipsilateral hand, wrist and elbow, nerve injury from fractures and carpal tunnel syndrome, or limb immobilization in casts, from transient decrease of blood supply to the nail matrix following trauma [Citation20]. When Beau’s lines are due to systemic causes, such as illness, severe stress, or systemic treatment, they affect all nails [Citation23] (). The distance of a Beau’s line from the proximal nail fold can estimate timing of the stressor [Citation22].
Figure 4. Clinical presentations of Beau’s lines, onychomadesis and retronychia. (A) Beau’s lines on the left toenails. (B) Onychomadesis of the left great toenail. (C) Retronychia of the right great toenail [Citation20].
Figure 5. 93-year-old female with bullous pemphigoid presented with Beau’s lines on all fingernails at even intervals coinciding with her monthly IVIG treatments [Citation23].
Onychomadesis is the complete nail plate separation and shedding with slow longitudinal growth rate. After a traumatic event, nail production may completely halt, leading to the loss of continuity between the nail plate and matrix. Hence, if the depression that is created from this event is deep enough, the nail will separate from the matrix and as the proximal nail grows out, it will wedge the distal plate up and eventually shed [Citation20].
Retronychia is the malalignment of the nail plate resulting in growth of the nail plate proximally toward the nail fold. It presents as overlapping layers of nails with no longitudinal growth. It most often affects the great toenails. Retronychia may result from repeated trauma, such as running or wearing ill-fitting footwear, or a single traumatic incident. Other causes include foot static disorders, such as reflex compensatory hyperextension of the halluces [Citation24]. There is a complete separation of the nail plate from the nail bed/matrix, with a new nail plate growing under the old one and pushing it into the nail fold, causing inflammation [Citation20]. Complications include pain, paronychia, granulation tissue, and nail bed shortening [Citation20].
Beau’s lines, onychomadesis, and retronychia are clinical diagnoses. Beau’s lines and onychomadesis will self-resolve once the inciting factor is removed. Patient education focuses on avoidance of trauma and keeping nails trimmed short. If retronychia is diagnosed within the first few months, patients are counseled to wear shoes with a wider toe-box to avoid toenail compression, and surgical nail avulsion may be curative. When retronychia is present for many years, treatment is challenging, and options include clobetasol ointment under occlusion to decrease inflammation and 40% urea under occlusion to chemically avulse the nail [Citation20].
Drug-Induced nail changes
Older patients often have medical conditions necessitating polypharmacy. Patients taking anti-inflammatory and anticoagulants such as aspirin or warfarin may develop subungual hemorrhages, affecting multiple nails in the absence of trauma [Citation25,Citation26]. Beta-blockers, such as propranolol, may cause digital gangrene in patients with severe peripheral vascular disease due to decreased perfusion and cardiac output due to beta-adrenergic receptor blockade [Citation25,Citation26]. Raynaud’s phenomenon may be the first sign of decreased perfusion, sometimes progressing to nail unit ischemia or necrosis [Citation26].
As there is an increased prevalence of cancer and polypharmacy among older adults, patients undergoing chemotherapy treatment may experience a variety of nail changes [Citation27]. Muehrcke’s lines are defined as opaque white transverse bands (apparent leukonychia) separated by normal pink colored nail, due to acute toxicity to tissues with high mitotic activity, such as the nail matrix. True transverse leukonychia is due to temporary impairment of distal nail matrix keratinocytes, and results in white opaque bands that are 1–2 mm wide, particularly with doxorubicin, cyclophosphamide, or vincristine. Beau’s lines, appear on all nails coinciding with timing of chemotherapy cycles. Other chemotherapy associated nail changes include longitudinal or transverse melanonychia due to activation of matrix melanocytes. Subungual hemorrhage and splinter hemorrhages may occur with taxanes and anthracyclines due to thrombocytopenia or blood extravasation. Hemorrhagic onycholysis and subungual abscesses occur in 44% of patients receiving taxanes, particularly docetaxel. Increased nail fragility and onycholysis may also occur. Paronychia with/without pyogenic granulomas are seen in association with chemotherapies including cetuximab/C225, osimertinib, and gefitinib [Citation25,Citation26,Citation28].
Infectious nail diseases
Onychomycosis
Onychomycosis is a common fungal infection of the nail unit, accounting for 50% of all nail disorders [Citation29]. It may be painful, cause psychosocial problems, lead to secondary infections and affect quality of life (QoL) [Citation30]. Prevalence increases with age [Citation31], and immunosuppression and diabetes mellitus are important risk factors [Citation32]. Clinical presentation includes yellow nail plate discoloration, thickening, onycholysis, crumbling, and subungual hyperkeratosis (). On dermoscopy, onychomycosis may present with a ruin-like appearance, longitudinal striae and spikes on the proximal margin of onycholytic areas, and the ‘aurora borealis’ sign which is chromonychia of multiple colors [Citation35]. There may be scaling of the plantar feet and/or interdigital spaces (tinea pedis). A nail clipping is imperative for mycological confirmation and accurate diagnosis, especially given that many older patients present with dystrophic nails due to a variety of conditions, including nail trauma and psoriasis [Citation29,Citation36–38].
Figure 6. Physical examination findings in onychomycosis. A, Right great toenail with subungual hyperkeratosis and nail plate onycholysis. B, Left great toenail with yellow discoloration and onycholysis. C, Multiple toenails with subungual hyperkeratosis and onycholysis. D, Toenails with severe onychodystrophy and ridging. E, Scale on the plantar feet and web spaces [Citation33].
Figure 7. Dermoscopy of onychomycosis. A, Fringed proximal margin of the onycholysis. B, Blurred yellow-orange-brown nail discoloration in longitudinal striae (the fading mimics Aurora Borealis). C, Distribution of the discoloration in longitudinal striae or round areas. D, Ruin-like appearance of the subungual scales that are white-yellow-orange in color. Photographs courtesy of Dr Maria Bianca Piraccini [Citation34].
There are three Food and Drug Administration (FDA) approved topicals and two FDA approved systemics options for onychomycosis treatment [Citation39]. Topicals include ciclopirox 8% lacquer, efinaconazole 10% solution and tavaborole 5% solution. FDA approved systemic agents include terbinafine and itraconazole [Citation29,Citation40]. Fluconazole is an off-label systemic treatment with broad-spectrum coverage [Citation40].
Advanced age is associated with lower cure rates, likely due to slower nail growth, poor circulation, and higher frequency of non-dermatophyte mold and mixed infections compared to younger individuals [Citation40]. Up to 20% of older patients with onychomycosis have other comorbid conditions and thus take multiple systemic medications which may interact with oral antifungals [Citation29,Citation41,Citation42].
Itraconazole has many drug-drug interactions as is a potent CYP3A4 inhibitor. Terbinafine is CYP2D6 inhibitor, but has few drug-drug interactions [Citation43]. Terbinafine is cleared both renally and hepatically, while itraconazole is cleared hepatically [Citation40]. Topical therapy would avoid systemic side effects and drug-drug interactions, but may be less effective due to inadequate nail plate penetration [Citation40]. Older adults may also have difficulty applying topicals if they have limited flexibility, visibility, or dexterity.
Periungual and subungual warts
Human papillomavirus (HPV) is responsible for nail unit verruca. Immunosuppression is an important risk factor [Citation5]. Treatment includes destructive modalities including electrocautery, cryosurgery, and ablative lasers [Citation44], and topicals, such as salicylic acid and imiquimod [Citation44]. Treatment of nail unit verruca is often challenging. Alternative therapies include intralesional (IL) candida antigen or bleomycin [Citation45,Citation46].
Acute paronychia
Acute paronychia is defined as a bacterial infection of the nail folds and is most commonly caused by Staphylococcus aureus. Patients often present with erythema, tenderness, and localized pus formation. The majority of acute paronychia cases are due to trauma and typically affect one nail [Citation3,Citation5]. Treatment is the same in all age groups and entails incision and drainage, warm saline soaks, and systemic or topical antibiotic therapy depending on sensitivities [Citation3].
Environmental nail changes
Chronic paronychia
Older adults may develop chronic paronychia, which is caused by nail fold inflammation (). Patients often present with erythematous and swollen nail folds with cuticle loss. In contrast to acute infections, patients may report discomfort, but are less likely to have pain [Citation3,Citation5]. Diagnosis is made via history and physical examination. Management requires irritant avoidance and keeping the digits dry. Medical treatment includes topical corticosteroids and antifungals. IL steroid treatment is sometimes used in recalcitrant cases [Citation3,Citation5].
Figure 8. Chronic paronychia presenting with edema of the right third and fourth nail folds. Of note, there is also benign longitudinal melanonychia of the right 4th fingernail.
Brittle nail syndrome (BNS)
Brittle nail syndrome (BNS) is defined as increased nail plate fragility and is most frequently seen in women and older patients [Citation47,Citation48]. It is theorized that decreased sulfur content in results in fewer disulfide bridges in proteins forming keratin fibrils [Citation4, Citation47]. The decreased cholesterol sulfate concentrations in nail clippings observed with increased age, may explain the increased incidence of BNS in older adults [Citation4,Citation49]. BNS presents with splitting (onychoschizia), onychorrhexis, or splitting (). Onychoschizia is due to decreased intercellular adhesion between nail plate corneocytes, and onychorrhexis is due to impaired nail matrix function [Citation4,Citation6]. While BNS is often idiopathic, it is often induced or worsened by frequent handwashing, regular manicures, and trauma. Diagnosis is based on history and clinical presentation. Differential diagnoses include trauma, nail psoriasis, and onychomycosis, which can be excluded with nail clippings. An underlying cause for BNS should be ruled out, such as vitamin C or iron deficiency, hypothyroidism, and chemotherapy [Citation50]. Treatment includes limiting contact with water and irritants, wearing gloves during wetwork, and applying nail strengtheners.
Figure 9. Clinical manifestations of brittle nail syndrome, including lamellar onychoschizia.
Inflammatory nail changes
Nail psoriasis
Nail Psoriasis (NP) is an inflammatory nail condition that may affect older patients, with a bimodal age incidence peaking at 30–39 and 60–69 years [Citation51]. A combination of environmental, genetic and immune stressors is involved in the pathogenesis. Nail matrix psoriasis presents with pitting, crumbling, leukonychia, and red spots in the lunula, while nail bed psoriasis presents with splinter hemorrhages, onycholysis, oil drops and nail bed hyperkeratosis [Citation52] (). Fingernails are more frequently affected than toenails [Citation51]. NP may present in isolation or more commonly with skin psoriasis. Nail pain is common, which can negatively impact QoL [Citation53]. A survey-based study of 2449 psoriasis patients using the Dermatology Life Quality Index showed that there was higher impair QoL in those with vs. without nail involvement (7.2 vs. 5.3; P.001) [Citation54]. Another survey-based study of 5400 psoriasis patients showed that NP decreased functionality most in putting on shoes or socks and household activities (21.2% and 25.1%, respectively), and caused pain in up to 35.8% of patients, further diminishing QoL [Citation55].
Figure 10. Nail pitting and onycholysis in right fingernails [Citation20].
Diagnosis is based on clinical history, physical examination, dermoscopy, and nail clippings. Joint examination and hand X-rays can help rule out psoriatic arthritis [Citation56]. Treatment for NP includes topicals or IL steroid matrical injections, which may be preferable when NP is isolated to a few nails [Citation49,Citation57]. Systemic therapies should be considered if NP is severe, involves many fingernails/toenails and with joint involvement [Citation57,Citation58]. Older adults are underrepresented in NP randomized clinical trials, thus recruitment of this population in research studies are needed to establish applicable NP treatment guidelines [Citation59].
Neoplastic nail changes
Nail unit melanoma
Nail unit melanoma (NUM) is a rare subset of cutaneous melanoma that is most frequently diagnosed between the ages of 50 and 70 years. The majority of NUM cases are located on either the thumb or hallux [Citation60].
Clinically, NUMs most commonly present as longitudinal melanonychia (LM), defined as a longitudinally oriented brown to black band that extends the length of the nail plate [Citation61] (). Up to 1/3 of NUMs are amelanotic, presenting as red nodules or longitudinal erythronychia with onycholysis, splitting, or ulceration [Citation63–65]. Concerning physical examination findings are bands measuring greater than 3 mm in width, band widening or heterogeneity in color, bleeding, and nail splitting [Citation62]. A Hutchinson’s sign, defined as periungual pigment involving the nail folds or hyponychium is often concerning for invasive melanoma [Citation63]. Diagnosis of NUM is often delayed due to varied presentation, lack of standardized clinical approach, poorly performed biopsies, or inaccurate interpretation of histopathology [Citation66].
Figure 11. Dermoscopic appearance of subungual melanomas. B, Brown lines on a brown background, irregular color, thickness, and spacing with no loss of parallelism. C, Brown lines on a brown background, irregular color, thickness, and spacing with loss of parallelism[Citation62].
NUM in situ can often be managed with en bloc excision that gives patients better QoL. Advanced NUM cases warrant amputation to avoid recurrence or metastases. The level of amputation at various joints is dependent on the degree of invasion into bone or joint spaces [Citation66]. Mohs micrographic surgery may be used as a digit-sparing technique for removal of NUM, and is most commonly used for tumors measuring less than 2 mm in depth [Citation63].
In addition to surgical management, individuals with more advanced cases of NUM may benefit from newer systemic therapies [Citation67]. These include programmed cell death protein-1 (PD-1) inhibitor monotherapy, lymphocyte activation gene-3 inhibitor (relatlimab) or cytotoxic T-lymphocyte associated antigen 4 (CTLA-4) inhibitor (ipilimumab) [Citation67]. Although these targeted therapies are currently the standard of care for cases of advanced cutaneous melanoma, there have been no clinical trials to date specifically analyzing response rates and outcomes in patients with NUM [Citation68].
Bowen’s disease
Bowen’s disease (BD), or squamous cell carcinoma in situ, rarely localizes to the nail unit and is most commonly diagnosed in men with peak incidence at 70 years [Citation69]. In a retrospective review of 120 HPV-associated nail unit BD cases, HPV subtype 16 DNA was identified by polymerase chain reaction in 74% of cases [Citation70]. Other risk factors include trauma, ionizing radiation, smoking, arsenic exposure, and chronic paronychia [Citation6,Citation71]. In a retrospective study of 12 cases of nail unit BD, 90% of patients were male, with mean age of onset 52 years. The thumb and middle finger were the most frequently affected digits (66%), and HPV infection was identified in 75% of cases [Citation71].
BD most commonly presents as an ulcerated hyperkeratotic lesion often accompanied by erythema, scaling, and crusting. Pigmented forms may mimic other nail conditions, including NUM, verruca, pyogenic granuloma, subungual exostosis, glomus tumor, or lichen planus [Citation69]. Diagnosis is often delayed due to its rarity and variable clinical presentation. Mohs micrographic surgery is the standard of care for treatment, which helps to preserve some nail unit and maintain digital function. Other nonsurgical treatment options include fluorouracil, imiquimod, photodynamic therapy, radiotherapy, carbon dioxide laser, but have lower clearance rates and higher recurrence rates compared to surgery [Citation6,Citation69].
Other nail changes
Myxoid cyst
Myxoid cysts affect the distal fingers and toes, and may be superficial (located near the proximal fold nail) or deep (located near the DIP joint). Clinically, they present as skin-colored to translucent, smooth, dome-shaped, and fluctuant nodules located distal to the interphalangeal joint, most commonly on the first three fingers [Citation34,Citation72] ().
They most frequently affect older adults and are often associated with osteoarthritis. In a cohort study of 51 patients with digital myxoid cysts, 74.5% showed radiologic evidence of primary interphalangeal joint osteoarthritis in affected digits [Citation34]. Due to their space occupying nature, they can influence the microvasculature, nail matrix function, nail shape and nail integrity. Consequently, when myxoid cysts are located near the proximal nail fold, they may compress the nail matrix resulting in a longitudinal groove [Citation74]. In a retrospective case series of 34 subungual myxoid cysts, increased transverse curvature (85%), lunular discoloration (76%), and nail splitting or partial destruction (44%) were most common [Citation74].
Asymptomatic myxoid cysts are best managed with clinical observation. Direct needle puncture with simple drainage and injection of corticosteroid may be attempted if symptomatic, although recurrence rates are high [Citation75]. Surgical excision is an alternative.
Conclusion
Nail conditions are common in geriatric patients and may impact their daily lives. Managing these conditions may be even more challenging in older adults due to limitations in their mobility dexterity when applying treatments. Moreover, even with proper diagnosis and treatment, resolution is often slow, since nails grow even more slowly in older adults. Examination of the toenails should be performed during the overall foot exam of older patients, especially considering that many comrobidities that affect older adults, such as diabetes, peripheral neuropathy, and peripheral artery disease, commonly involve the feet [Citation76]. As nail changes can physically and psychologically affect patients, it is important for physicians to diagnose and manage these nail conditions that can so easily go unrecognized in this expanding patient population.
Authors contributions
Author Albucker, Author Conway and Dr. Lipner contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
Acknowledgment
The authors thank the patients for providing their consents for the publication of their clinical photographs in this article.
Disclosure statement
Author Albucker, Author Conway and Dr, lipner have no relationships/activities/interests related to the content of the manuscript. Authors Albucker and Conway have no relevant conflicts of interest to disclose. Dr. Lipner has served as a consultant for Ortho Dermatologics, Hoth Therapeutics, and BelleTorus Corporation. No potential conflict of interest was reported by the author(s).
Ear eczema can be an extremely irritating and, at times, painful condition. It can range from slight dryness of the pinna (the visible, projecting part of the ear) to extensive skin loss and soreness, as well as infection of the external and internal parts of the ear. Eczema can affect the entire ear including the earlobes, conchal bowl (the area outside the ear hole), the ear opening (meatus), ear canal (also known as the external auditory canal – the part of the ear that leads to the ear drum) and the ear drum itself (also known as the tympanic membrane). The ear folds, backs of the ears and the area where the ears meet the face are also common areas for eczema.
Diagram showing parts of the ear
There are a number of causes of ear eczema and it is always best to consult your doctor if you think you may have it, in order to get effective treatment and prevent flare-ups. Several different types of eczema may affect the ear.
Atopic eczema
The ears and skin behind the ears are frequently affected in people with atopic eczema. As with other areas of the body, the eczematous skin here is dry, itchy and red or darker than a person’s usual skin colour, depending on skin tone. It can easily become infected, especially if the skin is scratched and breaks. A common site of ear eczema in people with atopic eczema is the junction between the earlobe and the face. Eczema in this area can cause painful cracks (fissures) in the skin, which can then easily become infected. Sometimes eczema can affect the whole of the pinna and track down the ear canal.
Seborrhoeic dermatitis
Seborrhoeic dermatitis is a form of eczema triggered by an over-reaction of the skin’s immune system to an overgrowth of a harmless yeast called malassezia that lives on the skin. People who have this type of eczema often have dandruff on the scalp and itchy, flaky skin with a yellowish, greasy scale in typical seborrhoeic dermatitis areas, which include the face (along the smile lines and eyebrows), centre of the chest and sometimes the eyelids and ears.
Around the ears, seborrhoeic dermatitis often takes the form of inflammation of the ear canal and along the hairline behind the ear (the post-auricular area), which can lead to painful fissures or cracks. It can sometimes be confused with psoriasis.
Treatment usually aims to reduce the overgrowth of yeast on the skin. This may include anti-fungal shampoos to wash the skin, and creams that may or may not contain mild topical steroids, such as Daktacort cream, to help reduce inflammation. Topical calcineurin inhibitors (Protopic ointment or Elidel cream) are sometimes used for this form of eczema, although they are not licensed for it.
Asteatotic eczema
This type of eczema affects older people. The exposed ear is vulnerable to changes in weather and temperature, which lead to dry, scaly and itchy skin causing asteatotic eczema. Aggravating factors include over-washing, cold or windy weather, central heating, low humidity indoors and air-conditioning.
Contact dermatitis
The external ear is commonly affected by both irritant and allergic contact dermatitis.
Irritant contact dermatitis comes about when the skin’s surface is irritated by a substance that causes the skin to become dry, itchy and red or darker than a person’s usual skin colour, depending on skin tone. Examples of substances that can cause irritant contact dermatitis around and inside the ears are shampoo, hair gel, hair spray, perm solution, hair colourant and perfume.
Allergic contact dermatitis develops as a result of your body reacting to a particular substance to which you are allergic. Everyday items that can cause allergic contact dermatitis around and inside the ears include the following:
Products used for the hair and scalp (for example, shampoo, conditioner, gel, hairspray, hair colourant, perm solution, hairpins and grips, hairnets and bathing caps). You might wish to try wearing ear plugs when showering and washing your hair, as these stop products collecting in the ear canal.
Earrings and studs, especially those containing nickel.
Plastic, rubber or metal ear appliances (for example, hearing aids and moulds, spectacles, head- and earphones, earbuds and earplugs).
Objects used to clean or scratch the ear.
Cosmetics and toiletries (for example, make-up, perfume and soap).
Topical medications (for example, ointments, creams and gels).
Allergens transferred to the ears via the fingers (for example, nail varnish and plant resin from poison ivy or oak).
Otitis externa
Also known as ‘swimmer’s ear’, this is an inflammatory condition of the ear canal. It can be caused by a primary skin problem, such as eczema, or by a bacterial or fungal infection. Having ear eczema increases your risk of getting otitis externa too. Other risk factors include swimming, sweating, high humidity and local trauma to the ear canal (for example, by using cotton buds or scratching the inside of the ear).
Symptoms include earache, skin becoming red or darker than your usual skin colour, depending on skin tone, swelling, itching and discharge from inside the ear. In severe cases, it can reduce people’s hearing due to swelling of the ear canal.
In suspected cases, dermatologists may seek help from the ear, nose and throat (ENT) medical team. To avoid getting otitis externa:
Keep the ear clean.
Avoid trauma, irritants and allergens.
Keep the outside of the ear dry – particularly after bathing and swimming.
Make sure any underlying contributing skin condition is well-controlled.
Ear piercing
Ear piercing does not cause ear eczema, but problems can occur later on as a consequence of wearing earrings or studs. Nickel allergy is very common and the chance of this developing is greatly increased if you have your ears pierced and if anything made even partly from nickel is worn in or on the ear.
If you definitely have a nickel allergy, wear only ‘hypo-allergenic’ jewellery or jewellery made from 18- carat gold, pure sterling silver, platinum or good-quality stainless steel. Foreign silver, rolled gold, white gold and gold plating should be avoided.
Pierced ears can become infected, particularly just after piercing. Make sure you go to a reputable ear-piercing technician to get your ears pierced, and wash the piercings frequently afterwards with the saline solution you were given by the ear-piercing technician.
Treatment of ear eczema
Treatment of ear eczema will depend on the cause and type of eczema, which will need to be diagnosed by your GP.
For atopic, seborrhoeic or asteatotic eczema, apply a medical emollient frequently to the affected areas. You may be prescribed a topical steroid for sore areas behind the ears, and in their folds. If you have seborrhoeic dermatitis, a topical steroid combined with an antifungal may be prescribed.
Topical calcineurin inhibitors, the brand names of which are Protopic and Elidel, are sometimes prescribed for ear eczema.
Apply your topical treatments by using a cotton bud to gently paint your cream or ointment on the affected area. Do not push the cotton bud into your ear.
If you have eczema inside the ear canal, you will need steroid drops, which will be prescribed by your GP or other healthcare professional.
If allergic contact dermatitis is suspected, you may be referred to a dermatology department to help find out what you are allergic to so that you can avoid it in the future. The dermatologist will usually recommend patch testing.
The usual treatment for otitis externa is antibiotic ear drops, which may also contain a steroid to reduce inflammation, itch and swelling. Sometimes a swab is taken to identify the most appropriate antibiotics – particularly if the condition does not improve. The ENT clinic may also clean the ear using gentle suction or irrigation (called ‘aural toilet’).
Cleaning of the ears and self-care
You can very gently wash the inside of your outer ear with water or preferably an emollient wash. You can also apply a damp cotton bud very gently to the bowl area of your ear but do not insert it into the ear canal. Never try to wash further into the ears – you can damage the skin of the ear canal by doing this.
After washing, dry your ears thoroughly. Using a warm (not hot) hairdryer is a good way to ensure your ears are dry. Avoid scratching the inside of your ears, especially with matches or hair grips – not only can these damage your ear canal skin or drum, but they may cause an allergic reaction after continuous use.
The use of ear candles is not advised as there is no evidence to suggest that they work, and they can damage the ears.
If you go swimming, use ear plugs. You can get custom-made ear moulds to fit your ears – they are like the moulds used for hearing aids. Ear moulds can be made and fitted at hearing aid centres. Larger chemists such as Boots provide this service, as do private audiologists.
Olive oil is sometimes recommended for moisturising around the ear pinna and loosening wax. However, medical research evidence shows that olive oil damages the skin barrier. Instead, we recommend applying an emollient to treat dry skin around the ears and in the entrance to the ear canals, and use refined petroleum oil (unfragranced baby oil) or sunflower oil to soften ear wax (but consult first with a healthcare professional). Water is not recommended, nor are wax softener products bought from chemists, as they may encourage the build-up of debris and cause more inflammation and irritation.
Infected ear eczema
Skin affected by eczema and dermatitis can become infected, usually by bacteria, especially if the skin surface is broken due to dryness and scratching. This is similar to eczema infections on other areas of the skin.
Ear eczema that becomes infected can encourage a build-up of wax, skin scales and hair in the ear canal, which can lead to blockage and cause temporary deafness. Infected eczema and ear infections can also come about when the ears are wet for long periods of time. For instance, if you swim a lot and leave your ears damp after swimming or washing your hair, your chances of an ear infection increase. Pressure from hearing aids and earpieces can also encourage ear infection, so try to ensure they are a comfortable fit.
Symptoms of infection inside the ear include earache, itching, pain, the skin becoming red or darker than your usual skin colour, depending on skin tone, weeping, swelling and an unpleasant smell or dirty-coloured discharge (often yellow or green) from inside the ear. If you have any of these signs, make an appointment to see your GP. Please note: ear discharge that is clear is normal if you have ear eczema, especially when eczema is active (weepy eczema).
You may be prescribed a ‘combination’ preparation containing a mixture of antibiotic and topical steroid for bacterial infections, or an antifungal and topical steroid for fungal infections. You should complete the course of treatment.
Aural toilet by healthcare professionals
A build-up of wax and flaky skin from patches of eczema can produce a lot of ‘debris’ in the ear canal. This can easily get infected, especially when water is present. So prevention of ear infection is key.
Manual cleaning of the ear by a healthcare professional is called ‘aural toilet’ and is often recommended to remove the debris and scale that can build up in the ear canal. It is done under a microscope, either using a pick or hook (Jobson Horne probe), or microsuction, an electric suction system.
Microsuction is also recommended if ear wax is truly impacted, and is considered safer and definitely better than flushing the ears with water, especially for people with ear eczema. Although many GP practices offer ear syringing and/or ear irrigation (an electronic machine for washing the ears) to remove ear wax, water-based methods are not recommended for people with ear eczema, unless it is very mild. Sometimes regular aural toilet is recommended (once or twice a year) to prevent wax and eczema debris build-up.
Aural toilet can be performed by aural care nurses/technicians, or sometimes by specially trained practice nurses. Ask your GP for a referral to the aural care service (provision may vary around the UK). Alternatively, this service may be provided privately by audiologists – your GP practice may be able to make a recommendation.
In summary
Ear eczema can be an extremely irritating condition and since it is difficult to look into the ears without specialist equipment, it is often hard to know what is going on, particularly in the case of young children.
If the ears become uncomfortable, don’t ignore it – it is always best to see your GP/healthcare professional, who can use a special torch to look inside. Often this will reveal the cause of ear discomfort and the problem can then be resolved, using one of the many treatments available for ear eczema and ear infections.




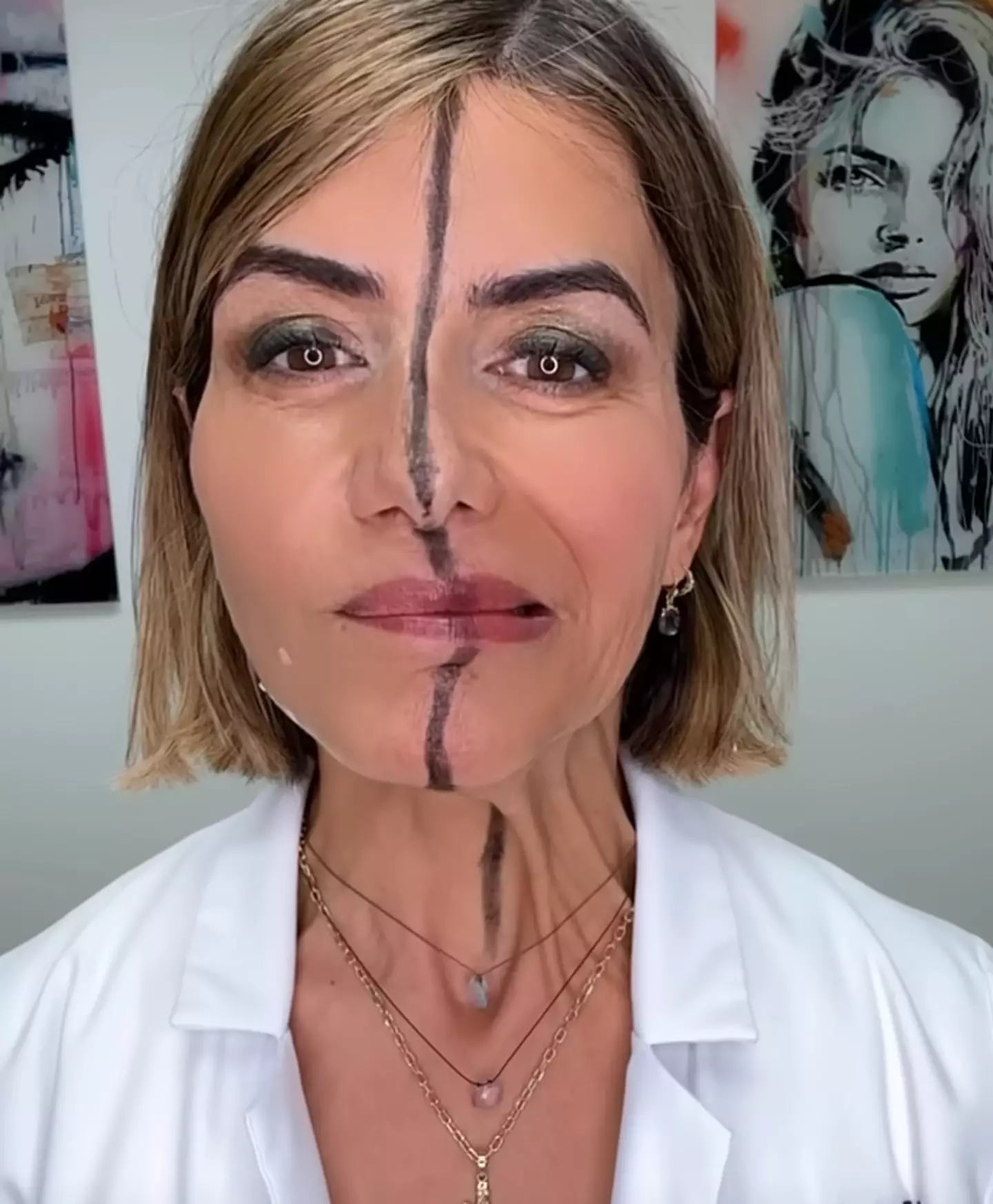






































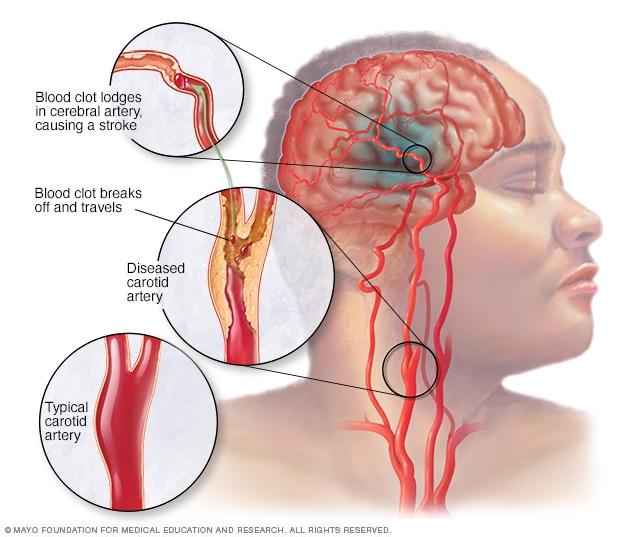
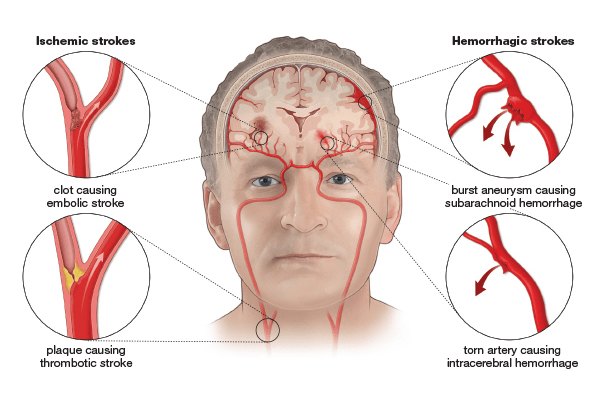

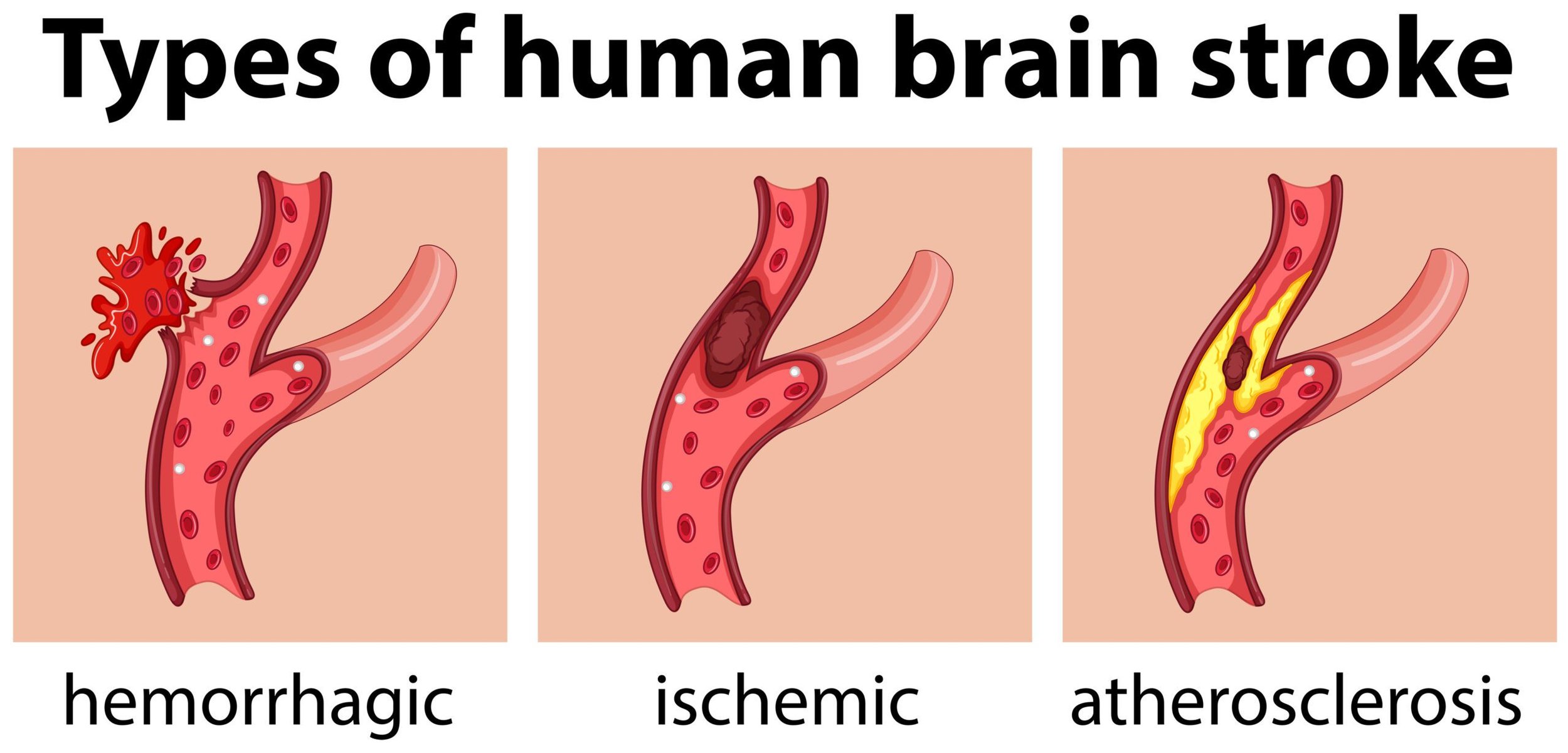
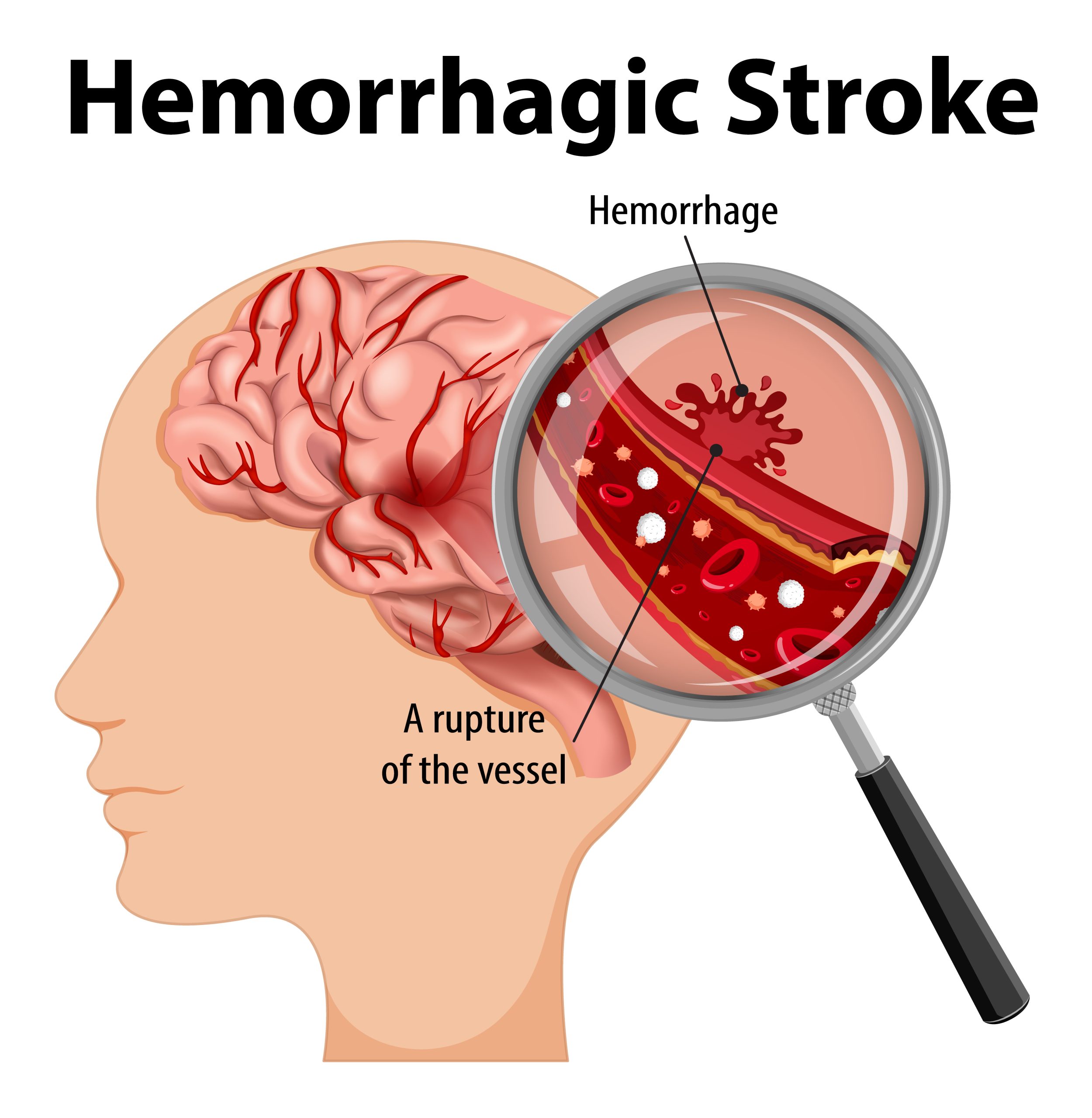
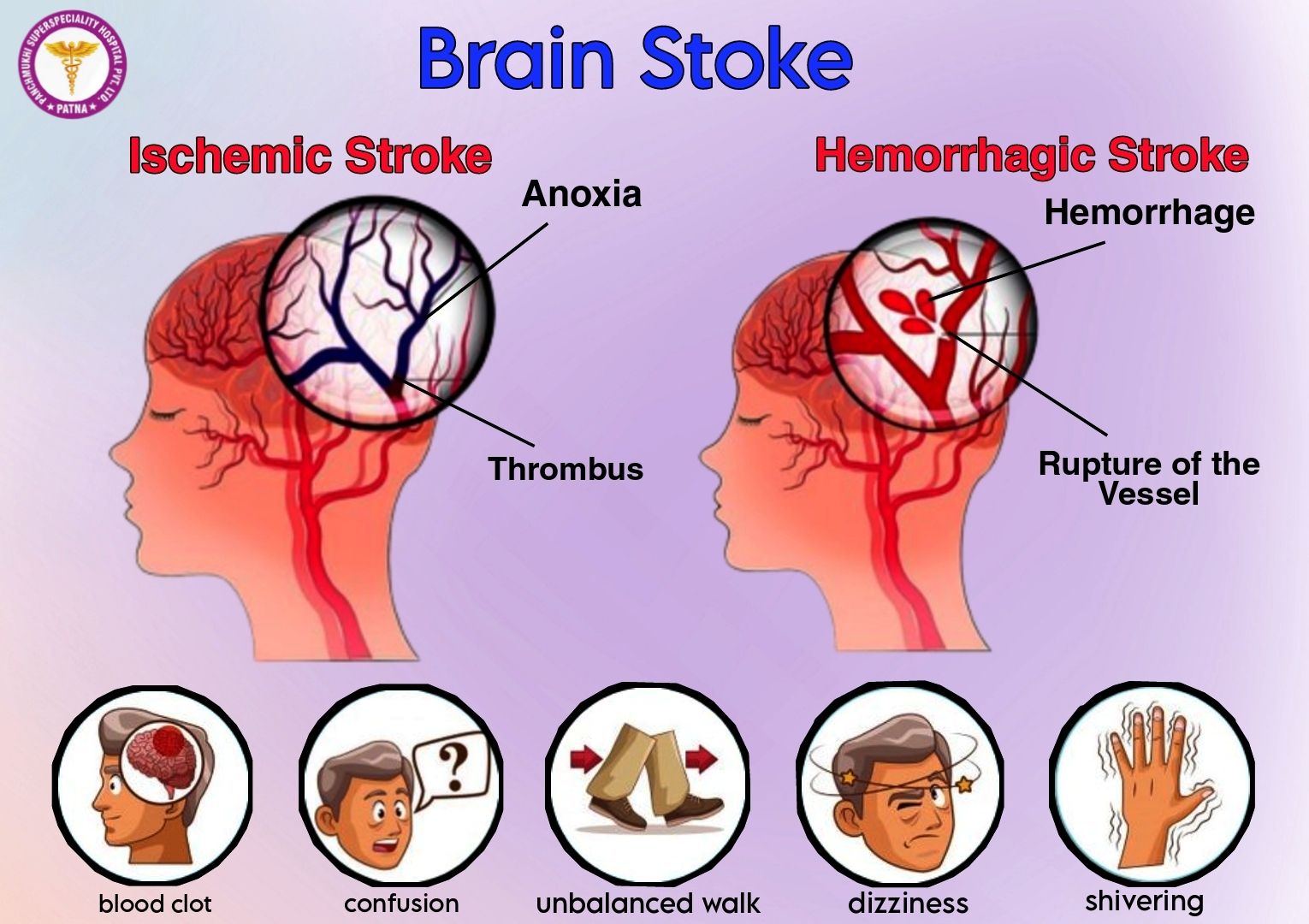




































![Figure 1. Pincer nail of the left first toenail in an 80-year-old woman. The lateral aspect of the nail plate is penetrating the periungual dermis of the lateral nail fold [Citation8].](https://www.tandfonline.com/cms/asset/b371fbc1-b699-4db4-925f-9fd76a8005b3/iann_a_2336989_f0001_c.jpg)
![Figure 2. A 75-year-old female presented with painful bilateral great toenails for 10 years. Her nails grew slowly and were extremely difficult to clip. A full nail examination was significant for opaque yellow-brown thickening, hyperkeratosis, elongation, and increased curvature of the great toenails. Onychogryphosis can be differentiated from retronychia and onychomycosis by its spiral striated appearance [Citation13].](https://www.tandfonline.com/cms/asset/37bfa230-31a9-4ea5-be2d-6213eb190967/iann_a_2336989_f0002_c.jpg)

![Figure 4. Clinical presentations of Beau’s lines, onychomadesis and retronychia. (A) Beau’s lines on the left toenails. (B) Onychomadesis of the left great toenail. (C) Retronychia of the right great toenail [Citation20].](https://www.tandfonline.com/cms/asset/28b7b61e-05eb-495a-8840-7852502e62e9/iann_a_2336989_f0004_c.jpg)
![Figure 5. 93-year-old female with bullous pemphigoid presented with Beau’s lines on all fingernails at even intervals coinciding with her monthly IVIG treatments [Citation23].](https://www.tandfonline.com/cms/asset/3aae46a7-e806-4a4b-8a85-7bb43bbf412a/iann_a_2336989_f0005_c.jpg)
![Figure 6. Physical examination findings in onychomycosis. A, Right great toenail with subungual hyperkeratosis and nail plate onycholysis. B, Left great toenail with yellow discoloration and onycholysis. C, Multiple toenails with subungual hyperkeratosis and onycholysis. D, Toenails with severe onychodystrophy and ridging. E, Scale on the plantar feet and web spaces [Citation33].](https://www.tandfonline.com/cms/asset/e92b5d45-1340-499a-b4bf-4f033e00cf45/iann_a_2336989_f0006_c.jpg)
![Figure 7. Dermoscopy of onychomycosis. A, Fringed proximal margin of the onycholysis. B, Blurred yellow-orange-brown nail discoloration in longitudinal striae (the fading mimics Aurora Borealis). C, Distribution of the discoloration in longitudinal striae or round areas. D, Ruin-like appearance of the subungual scales that are white-yellow-orange in color. Photographs courtesy of Dr Maria Bianca Piraccini [Citation34].](https://www.tandfonline.com/cms/asset/ebb4913a-53d9-49a3-aff4-ac5844a01c31/iann_a_2336989_f0007_c.jpg)


![Figure 10. Nail pitting and onycholysis in right fingernails [Citation20].](https://www.tandfonline.com/cms/asset/9660b1fb-2bbc-430f-9e27-9dcf72011b41/iann_a_2336989_f0010_c.jpg)
![Figure 11. Dermoscopic appearance of subungual melanomas. B, Brown lines on a brown background, irregular color, thickness, and spacing with no loss of parallelism. C, Brown lines on a brown background, irregular color, thickness, and spacing with loss of parallelism[Citation62].](https://www.tandfonline.com/cms/asset/74a5fabc-6954-4a49-83ce-75d6752880ac/iann_a_2336989_f0011_c.jpg)
![Figure 12. A, A translucent compressible nodule of the proximal nail fold and longitudinal groove in the nail plate of the right thumb. B, Transillumination using a dermatoscope to project light from the dorsal digit through the nail unit demonstrated a central nodule in the proximal nail fold as well as a second cyst radially. (Reprinted with permission from Cutis. 2020;105(2):82. ©2020, Frontline Medical Communications Inc.) [Citation73].](https://www.tandfonline.com/cms/asset/2e22d4d0-100e-4011-9cf8-89fbb8ab2381/iann_a_2336989_f0012_c.jpg)